

Evolving racial/ethnic disparities in AML survival in the novel therapy era
- PMID: 39888631
- PMCID: PMC11821405
- DOI: 10.1182/bloodadvances.2024014127
Evolving racial/ethnic disparities in AML survival in the novel therapy era
Abstract
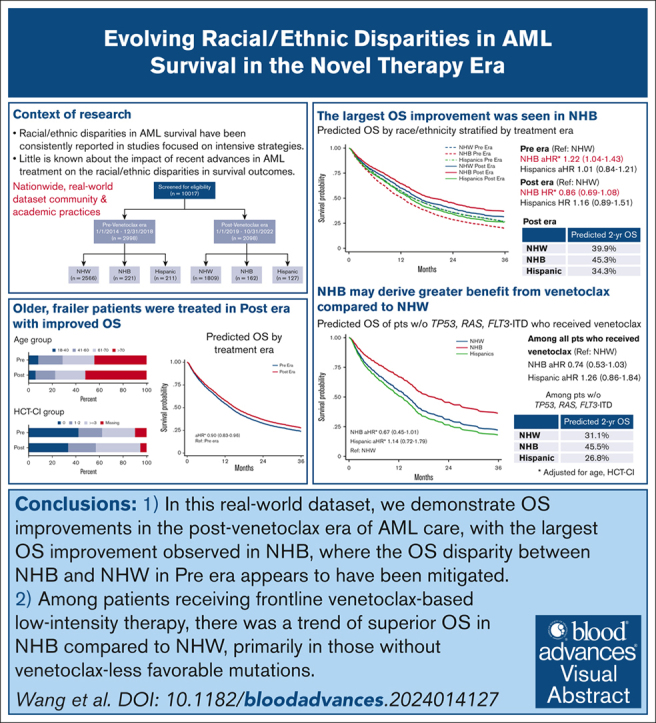
Little is known about the impact of recent advances in acute myeloid leukemia (AML) treatment on racial/ethnic disparities in survival outcomes. We performed a retrospective cohort study of patients with newly diagnosed AML using data from a nationwide electronic health record-derived deidentified database. Patients were categorized based on their diagnosis date relative to venetoclax approval, as pre-novel therapy era (Pre era; 2014-2018; n = 2998) or post-novel therapy era (Post era; 2019-2022; n = 2098). Patients in the Post era were older and had more comorbidities than Pre era. Non-Hispanic Black (NHB) and Hispanic patients were younger and more likely to have lower socioeconomic status than non-Hispanic White (NHW) patients, with no differences in the distributions of key disease features. After accounting for age and comorbidity, overall survival (OS) was higher in patients in Post era than Pre era (adjusted hazard ratio [aHR], 0.90; 95% confidence interval [CI], 0.83-0.96). In Pre era, NHB had a 22% higher hazard of death than NHW (aHR, 1.22; 95% CI, 1.04-1.43), whereas worse OS was not observed for NHB in Post era (aHR, 0.86; 95% CI, 0.69-1.08; predicted 2-year survival, 45.3% vs 39.9%). Utilization of novel therapeutics in frontline therapy did not differ by race/ethnicity. Among patients receiving venetoclax-based induction, particularly those without TP53, RAS, or FLT3-ITD mutations, results suggested higher OS for NHB than NHW patients (aHR, 0.67; 95% CI, 0.45-1.01). Additional studies are needed to elucidate factors contributing to these observed survival differences and to inform strategies to optimize outcomes for all patients with AML.
© 2024 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: S.M.L. received honoraria from Syros, Agios, Daiichi Sankyo, Jazz Pharmaceuticals, Brystol Myers Squibb (BMS), Acceleron, Astellas, and Pfizer, and research funding from Onconova, Celgene, Biosight, Hoffman-La Roche, and Kura. E.O.H. received research funding from Tmunity Therapeutics and Blueprint Medicines, and had membership on an entity's board of directors or advisory committees for Blueprint Medicines and PharmaEssentia. N.V.F. was a consultant for Sana Biotechnology, Kite Pharma, and Syndax Pharmaceuticals, and received research funding from Novartis. D.L.P. received honoraria from the American Society for Transplantation and Wiley and Sons Publishing; had membership on an entity's board of directors or advisory committees for American Society of Hematology, Decart, Incyte, Janssen, Kite/Gilead, National Marrow Donor Program, and Novartis; is a current equity holder in Genentech; and has patents and royalties with Unity. S.G. has licensed intellectual property with Novartis; received research funding from Novartis, Carisma Therapeutics, and Interius BioTherapeutics; and is a current holder of stock options in Carisma Therapeutics and Interius BioTherapeutics. I.M. received research funding from Genentech and Regeneron, and has reserved on an entity’s board of directors or advisory committees of Garuda Therapeutics. A.E.P. received research funding from Fujifilm, Daiichi Sankyo, Astellas, Arog, and AbbVie, and was a consultant for Daiichi Sankyo, Sumitomo Dainippon, Astellas, BMS/Celgene, Genentech, Loxo, Onconova, Syndax, Forma, Actinium, Roche, and AbbVie. K.W.P. has consulted for AbbVie, Agios, BMS, Astellas, and Novartis; received honoraria from AbbVie, BMS, Astellas, and Celgene; and received research funding from AbbVie, Astellas, and Millenium. C.L. served as a consultant for Taiho, Pfizer, Jazz, AbbVie, Rigel, BMS, Genentech, Novartis, Daiichi Sankyo, and Astellas, and has received research funding from Jazz. The remaining authors declare no competing financial interests.
Figures



References
-
- Patel MI, Ma Y, Mitchell B, Rhoads KF. How do differences in treatment impact racial and ethnic disparities in acute myeloid leukemia? Cancer Epidemiol Biomarkers Prev. 2015;24(2):344–349. - PubMed
-
- Patel MI, Ma Y, Mitchell BS, Rhoads KF. Age and genetics: how do prognostic factors at diagnosis explain disparities in acute myeloid leukemia? Am J Clin Oncol. 2015;38(2):159–164. - PubMed
-
- Sekeres MA, Peterson B, Dodge RK, et al. Differences in prognostic factors and outcomes in African Americans and whites with acute myeloid leukemia. Blood. 2004;103(11):4036–4042. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
