

Integrative proteo-transcriptomic characterization of advanced fibrosis in chronic liver disease across etiologies
- PMID: 39889710
- PMCID: PMC11866494
- DOI: 10.1016/j.xcrm.2025.101935
Integrative proteo-transcriptomic characterization of advanced fibrosis in chronic liver disease across etiologies
Abstract
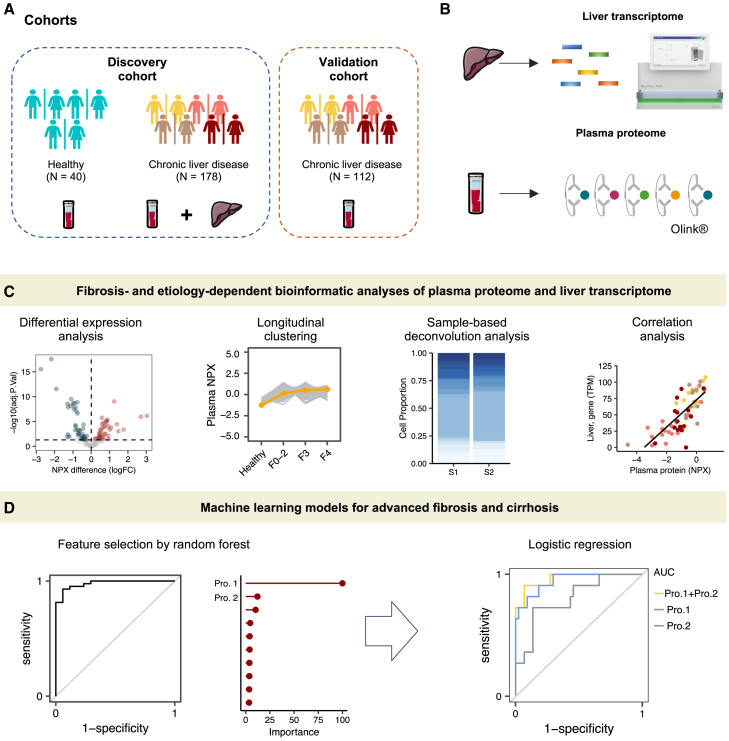
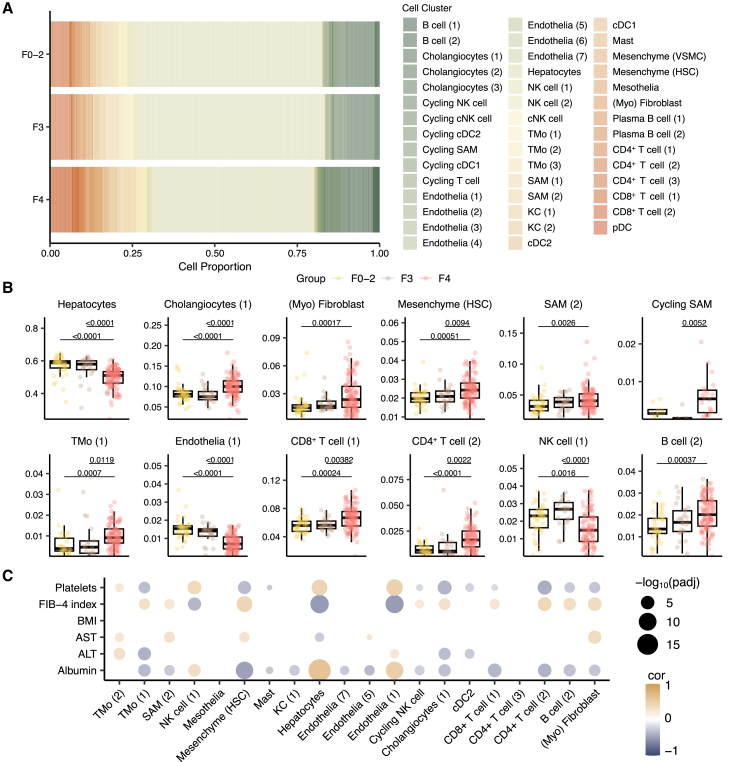
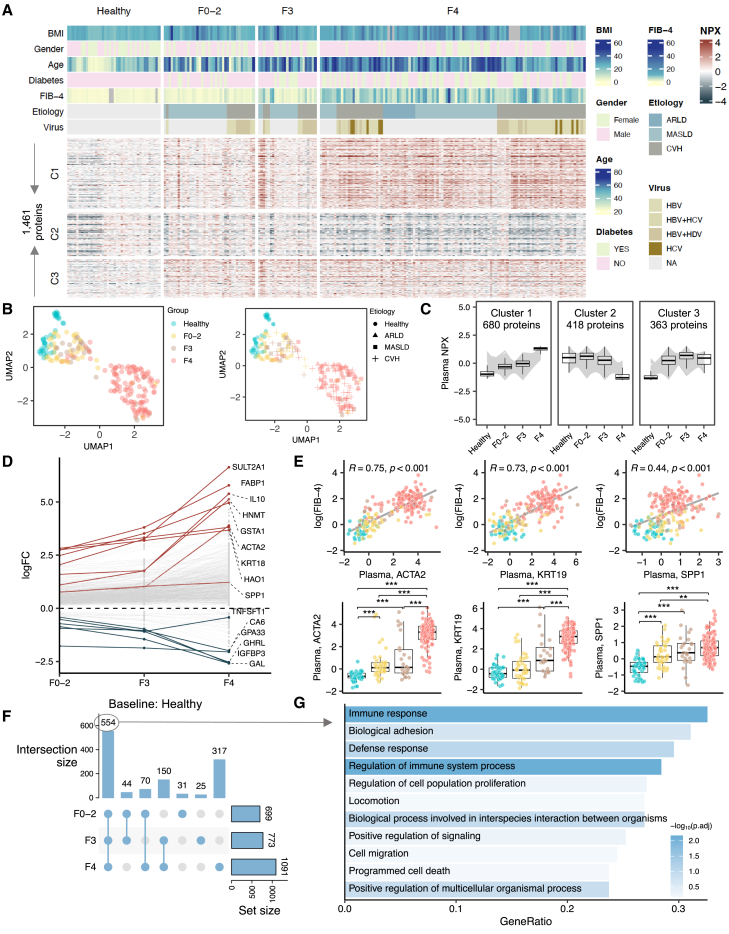
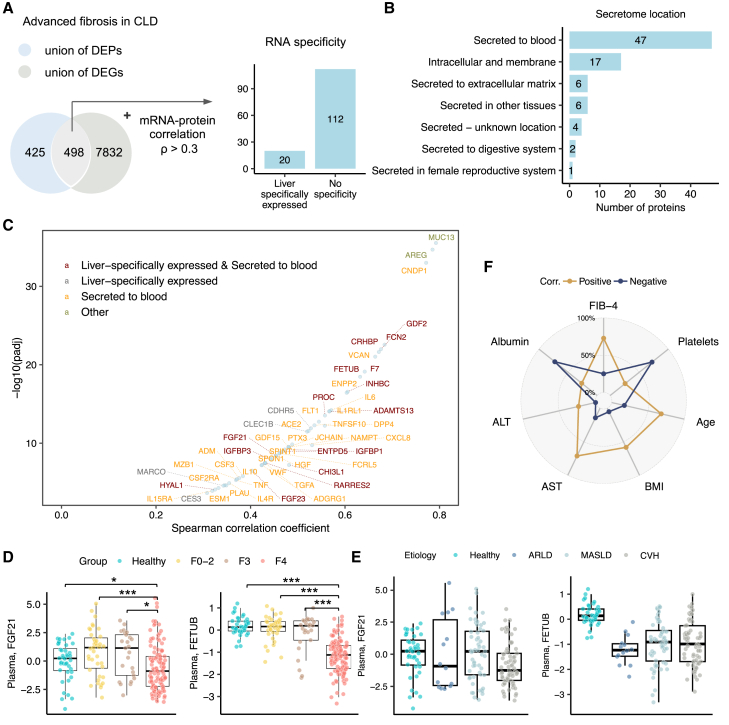
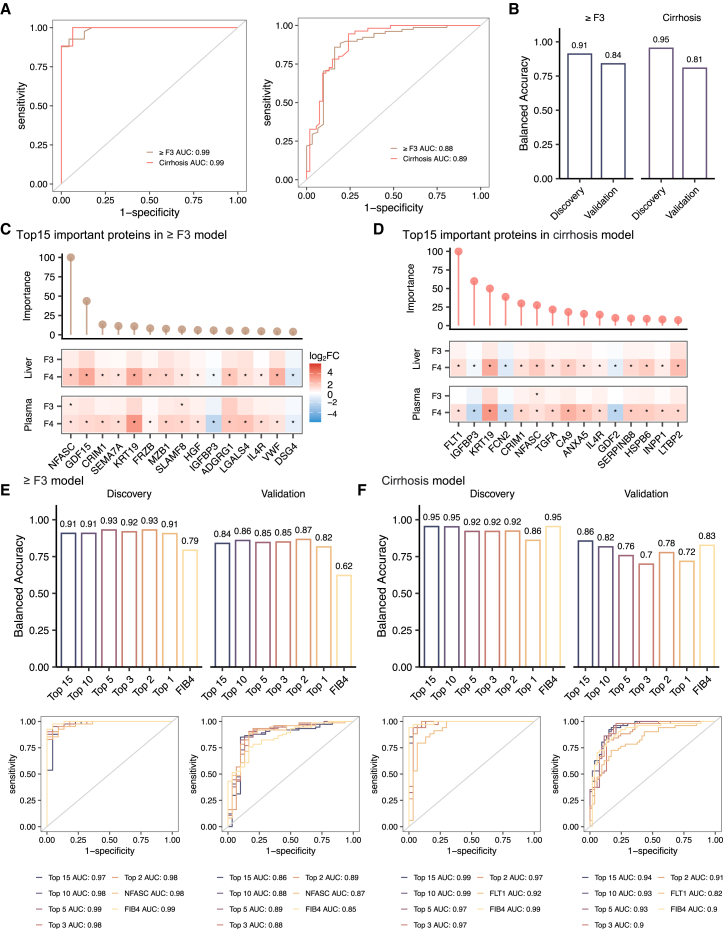
Chronic hepatic injury and inflammation from various causes can lead to fibrosis and cirrhosis, potentially predisposing to hepatocellular carcinoma. The molecular mechanisms underlying fibrosis and its progression remain incompletely understood. Using a proteo-transcriptomics approach, we analyze liver and plasma samples from 330 individuals, including 40 healthy individuals and 290 patients with histologically characterized fibrosis due to chronic viral infection, alcohol consumption, or metabolic dysfunction-associated steatotic liver disease. Our findings reveal dysregulated pathways related to extracellular matrix, immune response, inflammation, and metabolism in advanced fibrosis. We also identify 132 circulating proteins associated with advanced fibrosis, with neurofascin and growth differentiation factor 15 demonstrating superior predictive performance for advanced fibrosis(area under the receiver operating characteristic curve [AUROC] 0.89 [95% confidence interval (CI) 0.81-0.97]) compared to the fibrosis-4 model (AUROC 0.85 [95% CI 0.78-0.93]). These findings provide insights into fibrosis pathogenesis and highlight the potential for more accurate non-invasive diagnosis.
Keywords: chronic liver disease; liver fibrosis; multi-omics; non-invasive; systems biology.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.M., J.B., and M.U. are founders and shareholders of ScandiEdge and ScandiBio Therapeutics.
Figures


References
-
- Man S., Deng Y., Ma Y., Fu J., Bao H., Yu C., Lv J., Liu H., Wang B., Li L. Prevalence of Liver Steatosis and Fibrosis in the General Population and Various High-Risk Populations: A Nationwide Study With 5.7 Million Adults in China. Gastroenterology. 2023;165:1025–1040. doi: 10.1053/j.gastro.2023.05.053. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
