

The computerized algorithm for renal assessment improves diagnostic accuracy of renal impairment in hospitalized patients
- PMID: 39890827
- PMCID: PMC11785751
- DOI: 10.1038/s41598-025-87424-7
The computerized algorithm for renal assessment improves diagnostic accuracy of renal impairment in hospitalized patients
Abstract
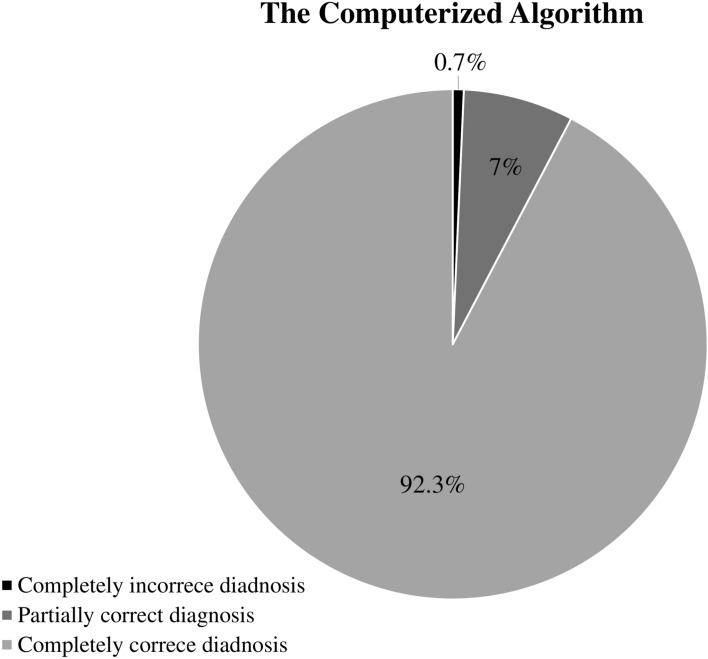
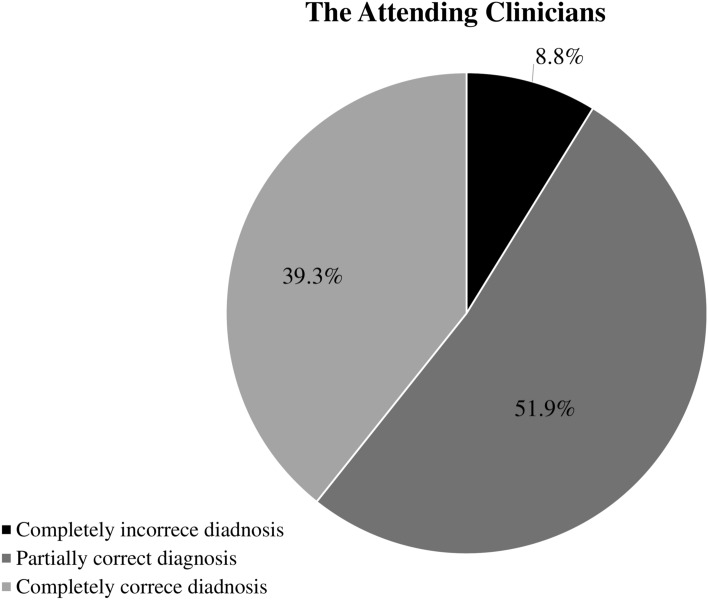
In hospitalized patients, acute kidney injury (AKI) is an important adverse event associated with high mortality and medical costs. Accurate diagnosis and timely management of AKI are essential for improving the outcomes of in-hospital AKI, and delayed diagnosis or misdiagnosis hinders advancements in AKI care. To ameliorate this problem, several electronic AKI alert systems have been proposed but have shown inconsistent effects on AKI outcomes. Before electronic systems can improve AKI outcomes, it is important to confirm their diagnostic accuracy. The purposes of the present study were to establish an easy-to-construct computerized algorithm for the diagnosis of renal impairment and to test its accuracy. The present study retrospectively included 1551 patients hospitalized in Wanfang Hospital with serum creatinine (SCr) levels > 1.3 mg/dL. A computerized algorithm was constructed to identify AKI events and chronic kidney disease (CKD) in these patients. Previous SCr tests were reviewed to define baseline SCr levels. A SCr level increased > 1.5 times from baseline was defined as AKI. An estimated glomerular filtration rate (eGFR) of < 60 mL/min/1.73 m2 for > 90 days was defined as CKD. Discharge diagnoses made by the attending physicians were defined as "clinician's diagnoses." The researcher's diagnoses, made by experienced nephrologists according to the same criteria, were the gold standard to which the computerized algorithms and the clinician's diagnoses were compared. The diagnoses made by the computerized algorithm and clinician were compared with the researcher's diagnoses to define their accuracy. Among the included patients, the mean age was 73.0 years; in-hospital mortality was 14.8%, and AKI was present in 28.6% of patients. Regarding the diagnostic accuracy for AKI, the computerized algorithm achieved a sensitivity of 85.6% and a specificity of 98.8%. The main cause of false-negative (FN) AKI diagnosis was AKI occurring prior to the outpatient visit, before the indexed hospitalization. Regarding the diagnostic accuracy for CKD, the computerized algorithm achieved a sensitivity of 94.7% and specificity of 100%. The main cause of FN CKD diagnosis was the lack of previous eGFR records. The computerized algorithm exhibited significantly superior accuracy compared to the clinician's diagnoses for both AKI (95.0% vs. 57.0%) and CKD (96.5% vs. 73.6%). We developed a simple and easy-to-construct computerized algorithm for the diagnosis of renal impairment that demonstrated significantly improved diagnostic accuracy for AKI and CKD compared to that of clinicians. In the future, an algorithmic approach for the differential diagnosis of AKI and a decision guide should be incorporated into this system.
Keywords: Acute kidney injury (AKI); Chronic kidney disease (CKD); Hospitalization; Intensive care unit (ICU).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
