

Balanced crystalloid versus saline for resuscitation in pediatric septic shock: a systematic review and meta-analysis
- PMID: 39891147
- PMCID: PMC11783956
- DOI: 10.1186/s12887-025-05442-w
Balanced crystalloid versus saline for resuscitation in pediatric septic shock: a systematic review and meta-analysis
Abstract
Background: Fluid resuscitation is a cornerstone of septic shock management in pediatric patients, with normal saline (NS) being the traditional choice. However, balanced solutions (BS) have gained attention due to their potential to mitigate acid-base and electrolyte disturbances. Despite this, the optimal choice between BS and NS for pediatric sepsis remains unclear. Therefore, we aimed to conduct a meta-analysis comparing the clinical outcomes of BS versus NS in pediatric patients with sepsis.
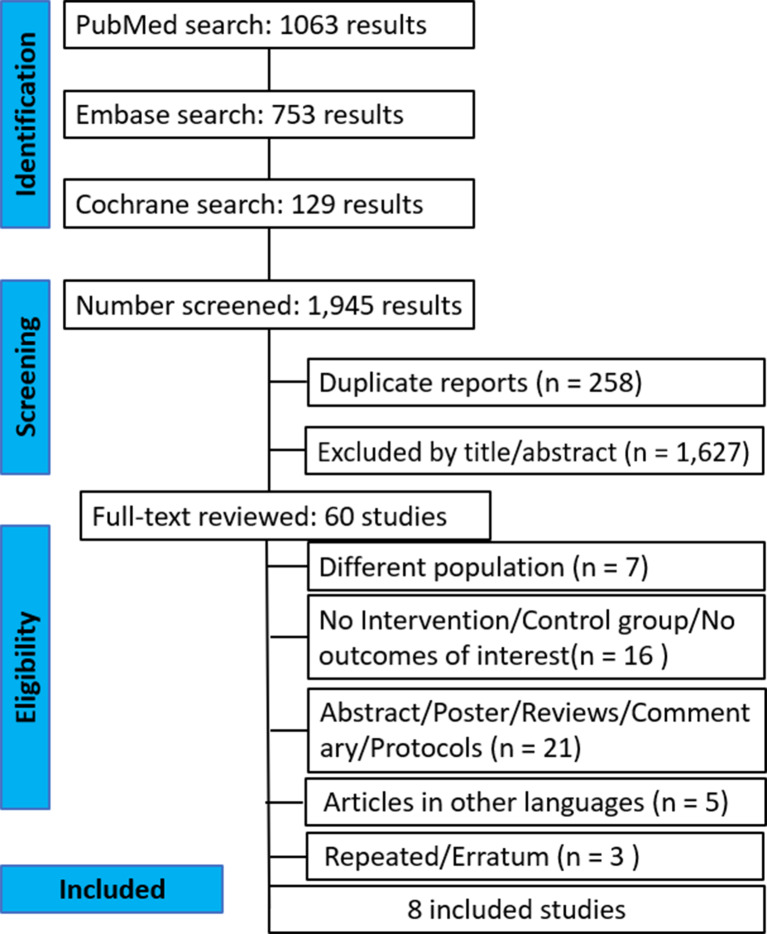
Methods: We systematically searched PubMed, EMBASE, and Cochrane Central Register of Controlled Trials, along with reference lists of retrieved publications, for studies comparing clinical outcomes in pediatric patients with sepsis treated with BS versus NS. Our outcomes of interest included acute kidney injury (AKI), hospital mortality, hospital length of stay, pediatric intensive care unit (PICU) length of stay, need for renal replacement therapy, hyperchloremia and mechanical ventilation. We performed statistical analysis using Review Manager Web 8.0.0 and Rstudio.
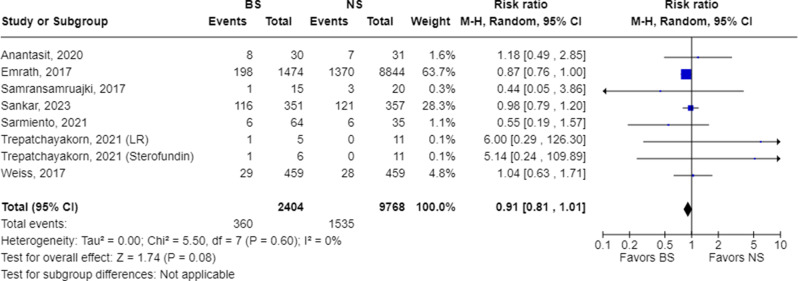
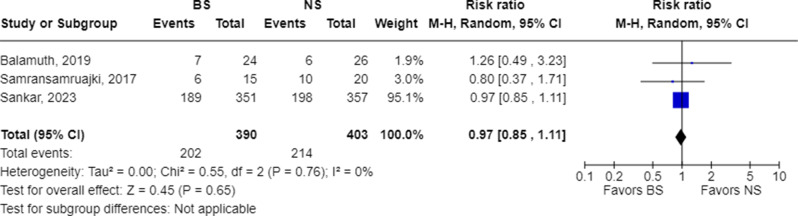
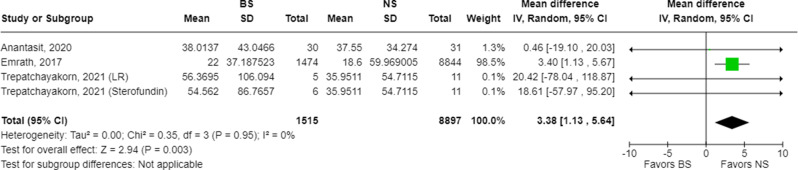
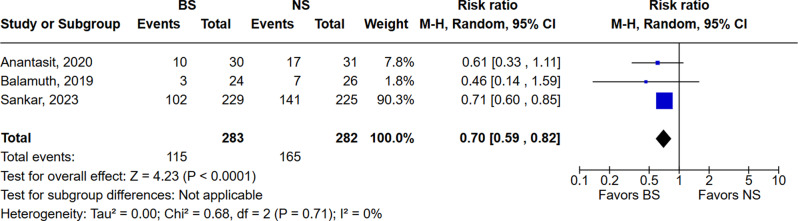
Results: We included 12,231 patients from 8 studies, of which 4 were randomized clinical trials (RCTs). BS was used to treat septic shock in 2,460 (20.1%) patients. The mean age was 5.98 ± 3.08 years, with 43.82% female patients. Follow-up ranged from 3 to 90 days. We found no statistically significant difference between groups in AKI, hospital mortality, mechanical ventilation, need for renal replacement therapy, and PICU length of stay. Hospital length of stay in days was significantly longer with BS compared to NS (MD 3.38; 95% CI 1.13 to 5.64; p = 0.003; I² = 0%) and the occurrence of hyperchloremia was lower in the BS compared to NS (RR 0.70; 95% CI 0.59 to 0.82; p = 0.0001; I² = 0%). In a subgroup analysis of RCTs only, AKI occurrence was not significantly different between BS and NS groups (RR 0.81; 95% CI 0.48 to 1.38; p = 0.44; I² = 18%). However, the need for renal replacement therapy was significantly less frequent in patients treated with BS compared to NS (RR 0.58; 95% CI 0.39 to 0.87; p = 0.008; I² = 0%).
Conclusion: In pediatric septic shock patients, treatment with balanced solutions (BS) was associated with a lower need for renal replacement therapy and a reduced occurrence of hyperchloremia. However, hospital length of stay was longer in patients treated with BS compared to those receiving normal saline (NS). These results underscore the complexity of fluid management in pediatric septic shock and emphasize the need for further research.
Keywords: Balanced solution; Crystalloid fluid; Normal saline; Pediatric; Ringer’s lactate; Septic shock.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Not applicable. Consent to participate: Not applicable. Consent to publish: Not applicable. Competing interests: The authors declare no competing interests. Disclosures: All authors report no relationships that could be construed as a conflict of interest. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Figures



References
-
- Global report on the Epidemiology and Burden of Sepsis: current evidence, identifying gaps and future directions. 1st ed. World Health Organization; 2020.
-
- Topjian AA, Raymond TT, Atkins D, et al. Part 4: Pediatric Basic and Advanced Life support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16suppl2):S469–523. 10.1161/CIR.0000000000000901. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
