

Blood-based prognostic scores and early dynamics under immunotherapy to select patients with metastatic solid tumors for continuing immune check-point inhibition: a prospective longitudinal study
- PMID: 39891724
- PMCID: PMC11787139
- DOI: 10.1007/s00262-024-03933-w
Blood-based prognostic scores and early dynamics under immunotherapy to select patients with metastatic solid tumors for continuing immune check-point inhibition: a prospective longitudinal study
Abstract
Introduction: Immune check-point inhibitors (ICI) were a major breakthrough in cancer care, but optimal patient selection remains elusive in most tumors.
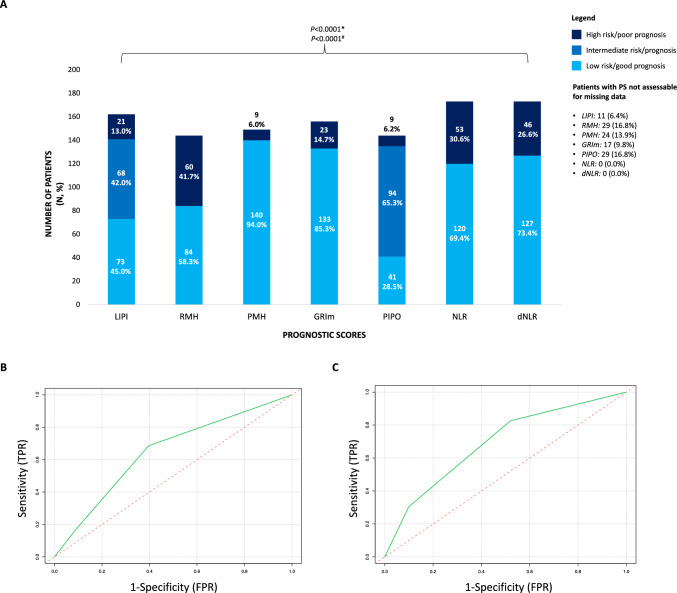
Methods: Overall 173 adult patients with metastatic solid tumors candidates to ICI in clinical trials at our Institution were prospectively recruited. Blood samples were collected at cycle 1 (C1D1) and 2 (C2D1) and until the occurrence of progressive disease (PD). C1D1 LIPI, RMH, PMHI, NLR, dNLR, PIPO and GRIm prognostic scores were calculated. The primary endpoint was identifying the best score to predict rapid PD (≤ 4 months) with ICI using logistic regressions accounting for tumor type, and receiving operators characteristics (ROC) with area under curve (AUC), accompanied by an extensive comparison of the score performances in the prediction of overall survival (OS), progression-free survival (PFS), overall response rates (ORR) and durable clinical benefit (DCB). Secondary objectives included describing study cohort outcomes and studying the association between the selected score at C1D1, C2D1 and its dynamics with OS and PFS.
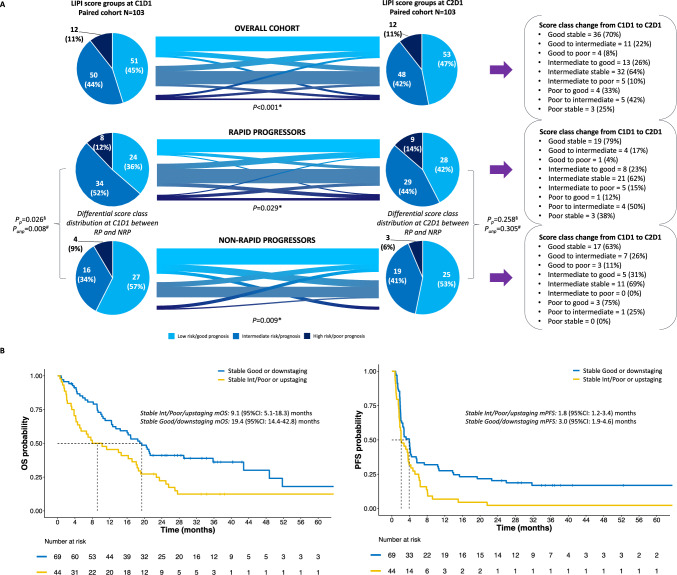
Results: C1D1 LIPI was the best predictor of rapid PD, OS and PFS, regardless of cancer type, compared to other scores. No score was associated to ORR and only RMH to DCB. Baseline LIPI detected three categories of patients with significantly different OS (p < 0.001) and PFS (p = 0.013). The same was observed at C2D1 for OS and PFS (both p = 0.020). Significant LIPI class shifts were observed in the overall population (p < 0.001), rapid progressors (p = 0.029) and non-rapid progressors (p = 0.009). Retaining a good LIPI or experiencing a shift towards a better prognostic class was associated to improved OS (p = 0.009) and PFS (p = 0.006). C2D1 LIPI, but not C1D1, remained significantly associated to rapid PD in multivariable analysis.
Conclusions: LIPI may improve patient selection for ICI and guide treatment adjustments according to on-treatment dynamics in a pancancer context.
Keywords: Cancer; Immune check-point inhibitors; Immunotherapy; LIPI score; Metastatic.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: J. García-Corbacho reports travel expenses from BMS and Pfizer and honoraria from Astra Zeneca, GSK, Lilly, Regeneron, Roche and Pfizer. L. Mezquita reports grants/research support from Amgen, Inivata, AstraZeneca and Gilead, honoraria/consultation fees from Roche, Takeda, Janssen and MSD, lectures and educational activities for Bristol-Meyers Squibb, Roche, Takeda, AstraZeneca, MSD, Radonova and Janssen, travel accommodation/expenses from Bristol-Meyers Squibb, Roche, Takeda, AstraZeneca and Janssen. F. Brasó-Maristany reports patent application (PCT/EP2022/086493, PCT/EP2023/060810, EP23382703 and EP23383369). N. Basté participated in advisory boards for Nanobiotix, Merck Serono, MSD, BioNtech, Roche, and BMS. T. Saurí served as a consultant at AstraZeneca, BMS, Roche, MSD, AMGEN, and Daiichi Sankyo and received lecture fees from BMS and MSD; B. Mellado reports research funding from Janssen, Roche, Bayer, and Pfizer; speakers’ bureau for Roche, Sanofi, Janssen, Astellas, Pfizer, Novartis, and Bristol-Myers Squibb; and travel and accommodation expenses from Janssen and Pfizer. Ò. Reig reports consulting or advisory role for BMS, EISAI, and Ipsen; and travel and accommodation expenses from Ipsen and Pfizer. L. Gaba reports advisory and consulting fees from GlaxoSmithKline, AstraZeneca, Merk Sharp Dohme, and PharmaMar, honoraria from GlaxoSmithKline, AstraZeneca, Merk Sharp Dohme, and PharmaMar for educational events/materials and travel expenses from GlaxoSmithKline, AstraZeneca, Merk Sharp Dohme. A. Prat reports advisory and consulting fees from AstraZeneca, Roche, Pfizer, Novartis, Daiichi Sankyo, and Peptomyc, lecture fees from AstraZeneca, Roche, Novartis, and Daiichi Sankyo, institutional financial interests from AstraZeneca, Novartis, Roche, and Daiichi Sankyo; stockholder and employee of Reveal Genomics; patents filed PCT/EP2016/080056, PCT/EP2022/086493, PCT/EP2023/060810, EP23382703 and EP23383369. F. Schettini reports honoraria from Novartis, Gilead, Veracyte and Daiichy-Sankyo for educational events/materials, advisory fees from Pfizer and Veracyte, and travel expenses from Novartis, Gilead and Daiichy-Sankyo. The other authors report no conflict of interest. Ethics approval and consent to participate: The study protocol was approved by the Ethic Committee of the HCB (IRB n. HCB/2017/0371) and was conducted according to the Declaration of Helsinki, good clinical practice guidelines and in compliance with applicable national and local laws. All patients signed an informed consent before entering the study.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
