

Comparison of airway pressure release ventilation (APRV) versus biphasic positive airway pressure (BIPAP) ventilation in COVID-19 associated ARDS using transpulmonary pressure monitoring
- PMID: 39893363
- PMCID: PMC11786409
- DOI: 10.1186/s12871-025-02904-7
Comparison of airway pressure release ventilation (APRV) versus biphasic positive airway pressure (BIPAP) ventilation in COVID-19 associated ARDS using transpulmonary pressure monitoring
Abstract
Background: APRV has been used for ARDS in the past. Little is known about the risk of ventilator- induced lung- injury (VILI) in APRV vs. BIPAP in the management of in COVID19-associated ARDS (CARDS). This study aimed to compare transpulmonary pressures (TPP) in APRV vs. BIPAP in CARDS in regard to lung protective ventilator settings.
Methods: This retrospective, monocentric cohort study (ethical approval: 21-1553) assessed all adult ICU- patients with CARDS who were ventilated with BIPAP vs. APRV and monitored with TPP from 03/2020 to 10/2021. Ventilator-settings / -pressures, TPP, hemodynamic and arterial blood gas parameters were compared in both modes.
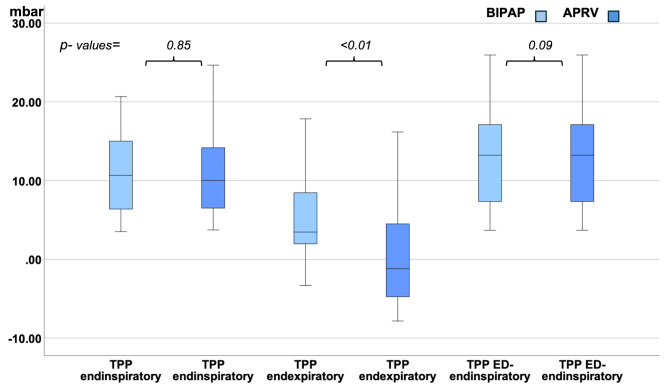
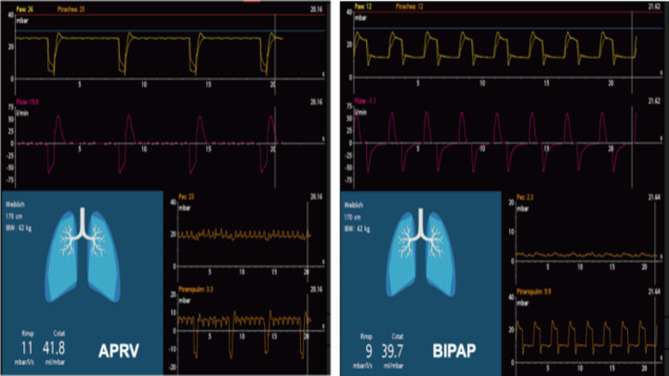
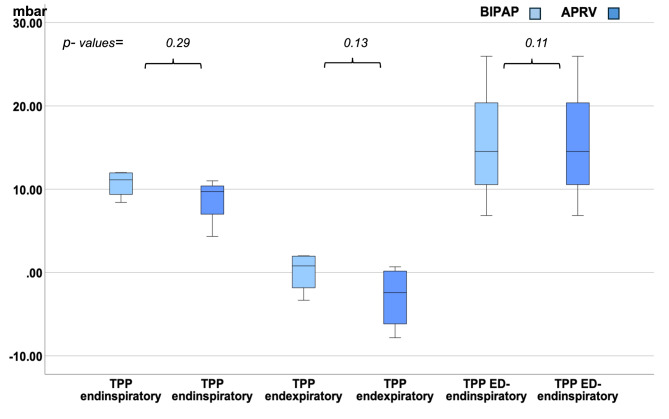
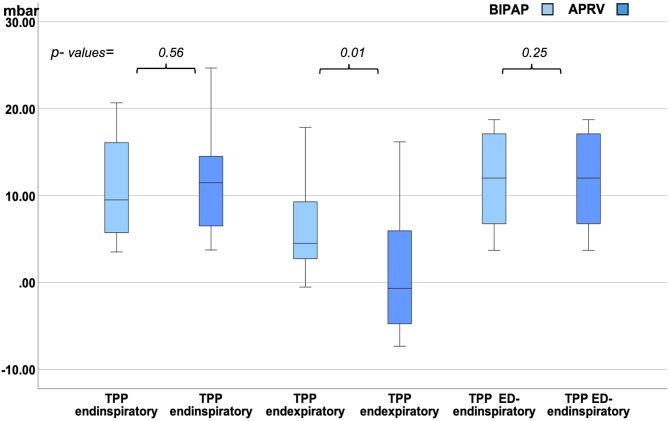
Results: 20 non- spontaneously breathing patients could be included in the study: Median TPPendexpiratory was lower / negative in APRV (-1.20mbar; IQR - 4.88 / +4.53) vs. positive in BIPAP (+ 3.4mbar; IQR + 1.95 / +8.57; p < .01). Median TPPendinspiratory did not differ. In APRV, mean tidal- volume per body- weight (7.05 ± 1.28 vs. 5.03 ± 0.77 ml; p < .01) and mean airway- pressure (27.08 ± 1.67 vs. 22.68 ± 2.62mbar; p < .01) were higher. There was no difference in PEEP, peak-, plateau- or driving- pressure, compliance, oxygenation and CO2- removal between both modes.
Conclusion: Despite higher tidal- volumes / airway-pressures in APRV vs. BIPAP, TPPendinspiratory was not increased. However, in APRV median TPPendexpiratory was negative indicating an elevated risk of occult atelectasis in APRV- mode in CARDS. Therefore, TPP- monitoring could be a useful tool for monitoring a safe application of APRV- mode in CARDS.
Keywords: APRV; ARDS; Atelectrauma; BIPAP; CARDS; COVID; SARS CoV-2; Transpulmonary pressure; VILI; Ventilator associated lung injury.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of the University of Cologne, Germany (21-1553-retro) as a low risk with a waiver of individual patient informed consent due to the retrospective character and the analysis of pseudonymized data. Informed consent was not taken from the individual patient. The study was conducted according to the declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
