

Opioid sparing anesthesia in patients with liver cirrhosis undergoing liver resection: a controlled randomized double-blind study
- PMID: 39893417
- PMCID: PMC11786452
- DOI: 10.1186/s12871-025-02915-4
Opioid sparing anesthesia in patients with liver cirrhosis undergoing liver resection: a controlled randomized double-blind study
Abstract
Objective: Opioid metabolism and pharmacodynamics may be affected in hepatic patients. Ketamine and dexmedetomidine are conventional anesthetics used in our daily practice. The opioid-sparing effects of this combination have not been evaluated in patients with liver cirrhosis undergoing liver resection. We aimed to investigate the potential peri-operative opioid-sparing effects of intra-operative dexmedetomidine and ketamine infusions in patients with Child A liver cirrhosis undergoing liver resection.
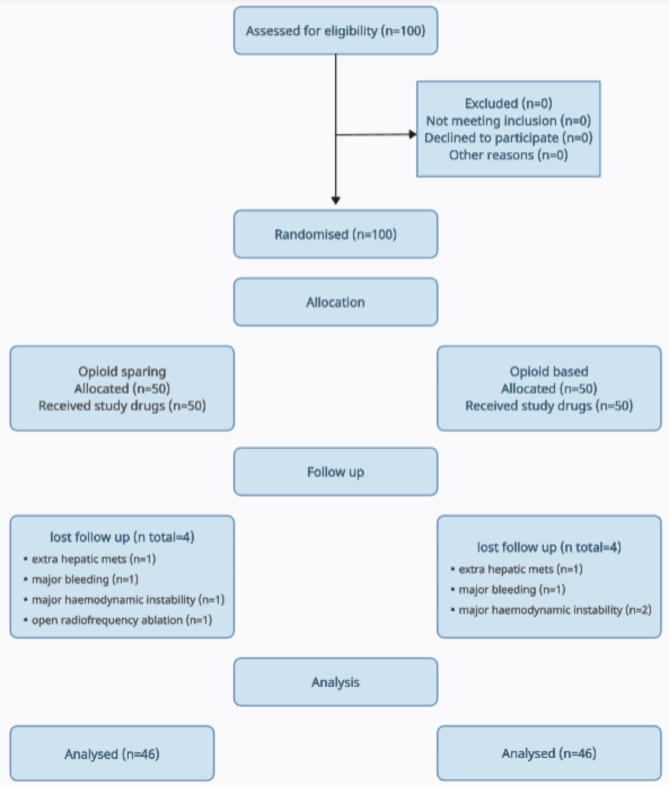
Methods: This study was a randomized controlled double-blind trial. 92 adult patients of both sex with Child class (A) liver cirrhosis aged 18 to 65 years entering and completing the study. We excluded patients with renal or cardiac dysfunction or contraindications from study medications.46 patients in the opioid-sparing group (OS) receiving ketamine and dexmedetomidine infusions and 46 patients in the opioid-based (OB) group as controls. The main outcome measures: were intra-operative fentanyl requirements, postoperative fentanyl requirements, visual analogue pain scores, postoperative nausea, vomiting, ileus, desaturation, intra-operative hemodynamic events, and ICU stay were recorded.
Results: The total intra-operative fentanyl consumption was significantly lower in the OS group compared with the OB group, 183.2 ± 35.61 µg and 313.5 ± 75.06 µg, respectively, P < 0.001. The postoperative 1st 48 h fentanyl consumption was significantly lower in the OS group compared with the OB group, 354.5 ± 112.62 µg and 779.1 ± 294.97 ± µg, respectively, P < 0.001. Visual analogue scores were significantly better in the OS group at the early 2-hour assessment point postoperatively. The postoperative adverse events were significantly more frequent in the opioid-based group. ICU stay was significantly shorter in the OS group.
Conclusions: Administering dexmedetomidine and ketamine infusions intra-operatively to patients with Child A liver cirrhosis undergoing liver resection resulted in notable opioid-sparing effects, with reductions of approximately 40% intra-operatively and 55% postoperatively. The opioid-sparing group exhibited improved postoperative outcomes, including reduced pain, decreased incidence of opioid-related side effects and shorter ICU stays.
Keywords: Liver cirrhosis; Liver resection; OSA.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for this study (Ethical Committee N° 00309/2022) was provided by the Institutional Review Board of the National Liver Institute, Written informed consent was obtained from all participants. Consent for publication: Not applicable. Clinical registration: The study was registered in the ClinicalTrials.gov identifier number: NCT05674877. Competing interests: The authors declare no competing interests.
Figures
References
-
- Roberts GW, Bekker TB, Carlsen HH, Moffatt CH, Slattery PJ, McClure AF. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg. 2005;101:1343–8. 10.1213/01.ANE.0000180204.64588.EC. - PubMed
-
- Mauermann E, Filitz J, Dolder P, Rentsch KM, Bandschapp O, Ruppen W. Does fentanyl lead to opioid-induced hyperalgesia in healthy volunteers? A double-blind, randomized, crossover trial. Anesthesiology. 2016;124:453–63. 10.1097/ALN.0000000000000976. - PubMed
-
- Oderda GM, Gan TJ, Johnson BH, Robinson SB. Effect of opioid-related adverse events on outcomes in selected surgical patients. J Pain Palliat Care Pharmacother. 2013;27:62–70. 10.3109/15360288.2012.751956. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
