

The value of fixed segment mobility in posterior dynamic stabilization: a single-center retrospective study
- PMID: 39893433
- PMCID: PMC11786513
- DOI: 10.1186/s12891-025-08333-4
The value of fixed segment mobility in posterior dynamic stabilization: a single-center retrospective study
Abstract
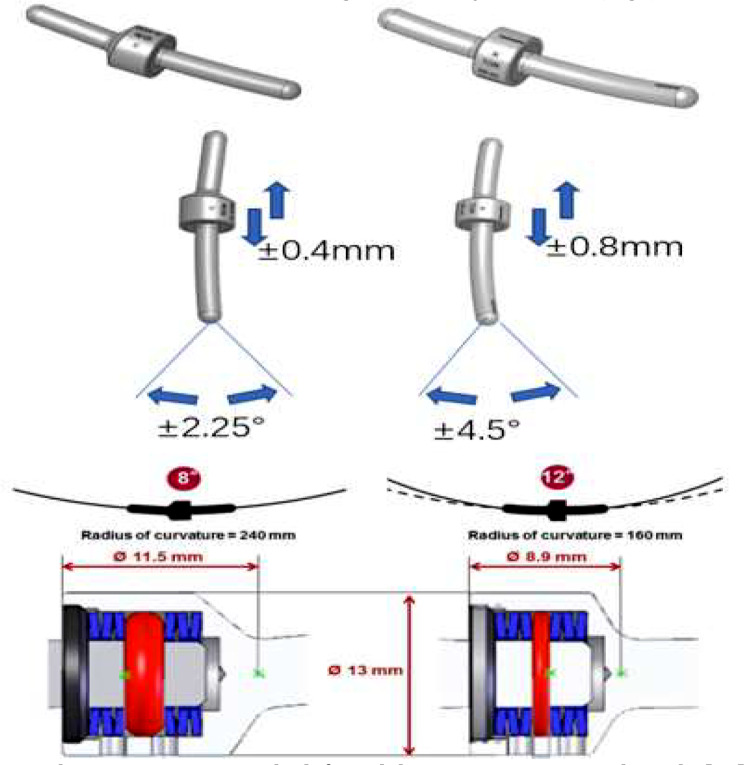
Purpose: This study aims to compare the effects of two generations of the Isobar dynamic fixation system-Isobar TTL (first-generation, less mobile) and Isobar EVO (second-generation, more mobile)-on the surgical and adjacent intervertebral disc segments, based on MRI findings.
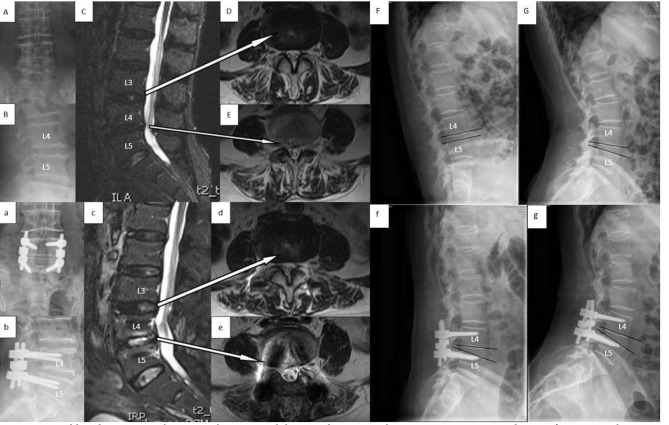
Methods: A retrospective analysis was conducted on 29 patients treated with fenestrated decompression and Isobar EVO stabilization and 34 patients treated with fenestrated decompression and Isobar TTL stabilization. Clinical outcomes and radiographic parameters, including the disc height index (DHI) and range of motion (ROM) of the surgical and upper adjacent segments, lateral neural foraminal protrusion value (LNPV) of the upper adjacent segment, and Pfirrmann grading of disc degeneration, were evaluated and compared between the two groups.
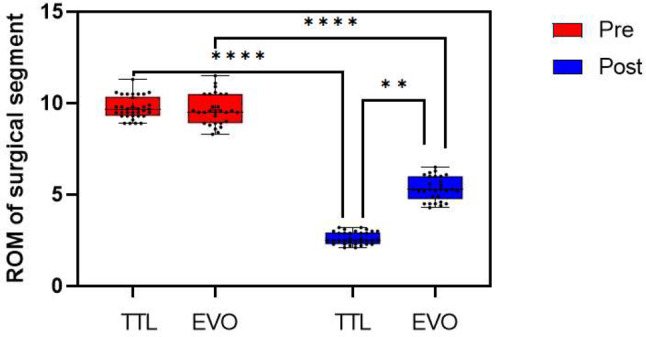
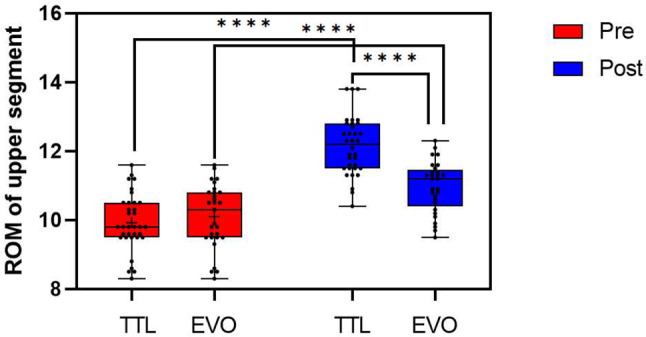
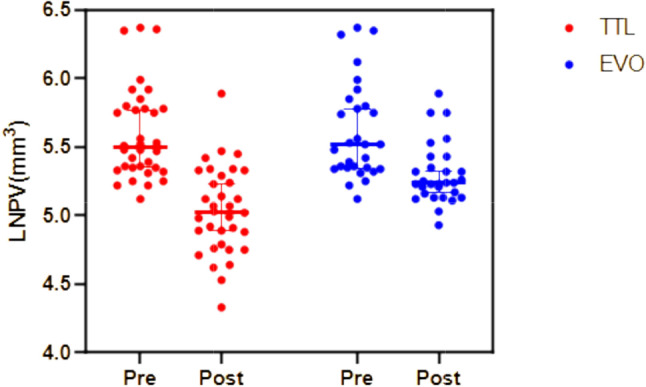
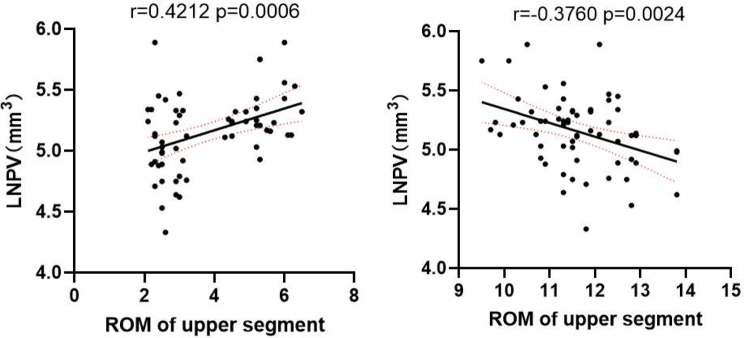
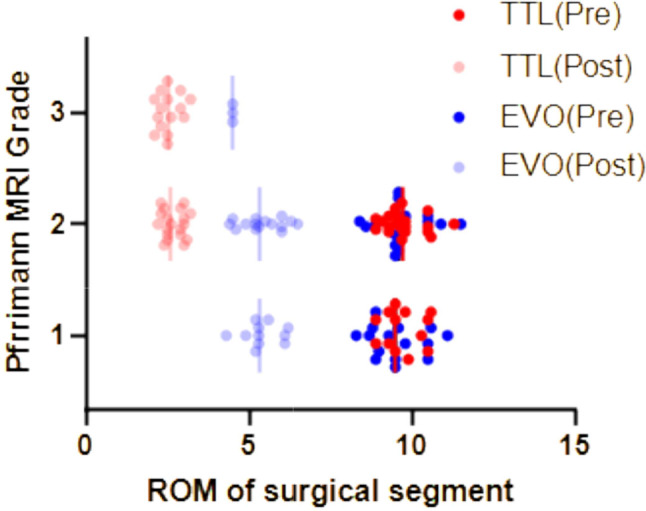
Results: At the 48-month follow-up, no significant differences in Visual Analog Scale (VAS) scores or Oswestry Disability Index (ODI) were observed between the two groups (P > 0.01). The EVO group demonstrated significantly higher surgical segment DHI and ROM compared to the TTL group (P < 0.01). Meanwhile, the upper adjacent segment ROM was significantly lower in the EVO group compared to the TTL group at the final follow-up (P < 0.01). Additionally, the upper adjacent segment LNPV was larger in the EVO group than in the TTL group (P < 0.01). Pfirrmann grading revealed greater degeneration in surgical segments treated with TTL compared to EVO (P = 0.008).
Conclusion: Compared to the first-generation, less mobile Isobar TTL, the second-generation, more mobile Isobar EVO offers superior preservation of the surgical segment and slows the progression of degeneration in the upper adjacent segments. These findings highlight the benefits of greater mobility in posterior dynamic stabilization devices.
Keywords: Adjacent segment degeneration; Dynamic stabilization; Isobar system; Lumbar degenerative diseases; Non-fusion.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: We declare that the study has been performed in accordance with the Declaration of Helsinki and has been approved by the institutional review board of Affiliated Hospital of Shaanxi University of Chinese Medicine. All patients participated freely and with written informed consent to the study. Consent for publication: The authors declare that there are no conflicts of interest regarding the publication of this paper. Competing interests: The authors declare no competing interests.
Figures


References
-
- Li CH, Zhao H, Yu X. er al(2019). The research status and progress of impact of pre-existing adjacent segment pathology on adjacent segment degeneration after lumbar spinal fusion[J]. Orthopaedic Biomechanics Materials and Clinical Study,16(3):67–70. 10.3969/j.issn.1672-5972.2019.03.015
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
