

Carpal Kinematics in the Normal, Scapholunate Ligament Deficient, and Surgically Reconstructed Wrist
- PMID: 39893567
- PMCID: PMC11898162
- DOI: 10.1002/jor.26049
Carpal Kinematics in the Normal, Scapholunate Ligament Deficient, and Surgically Reconstructed Wrist
Abstract
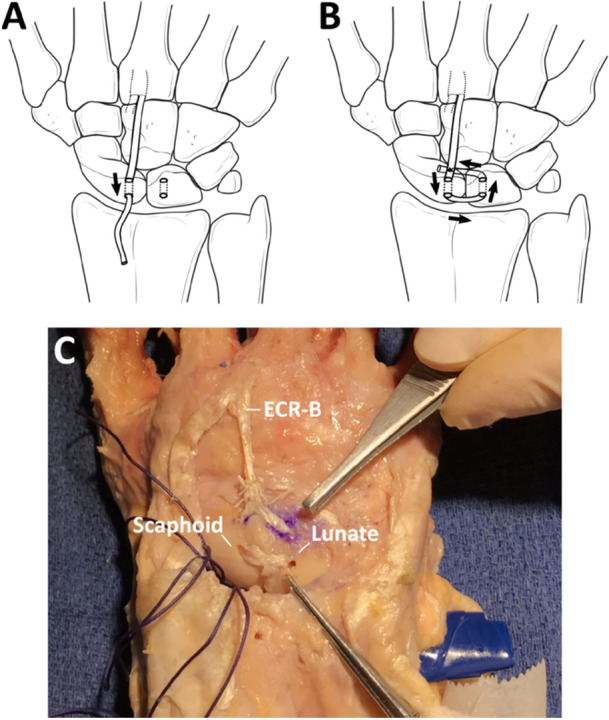
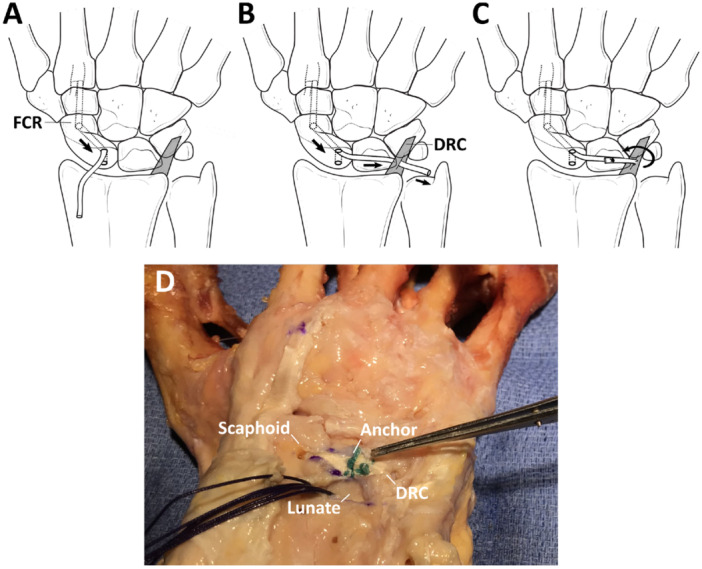
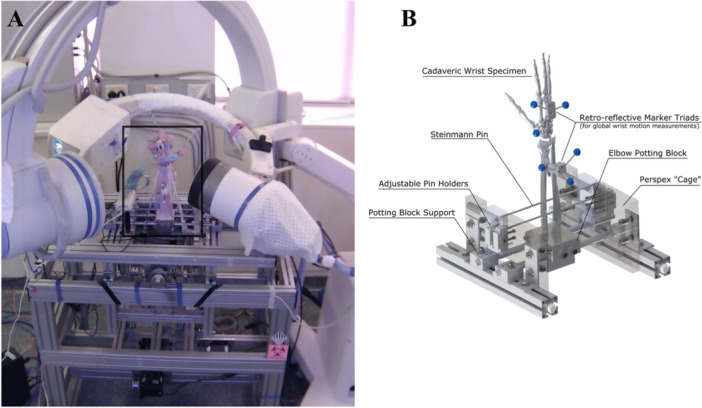
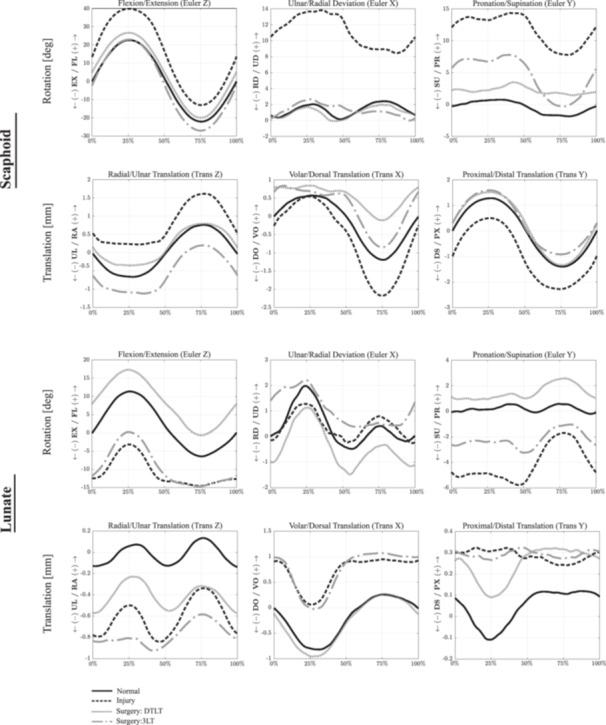
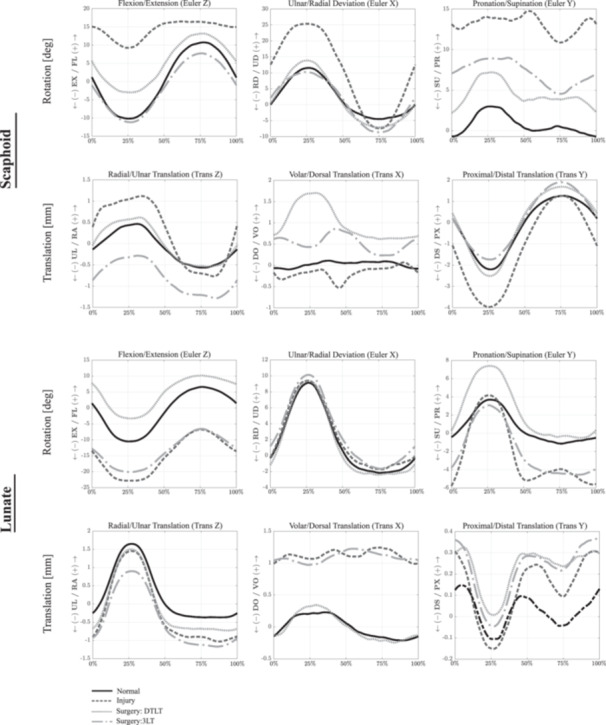
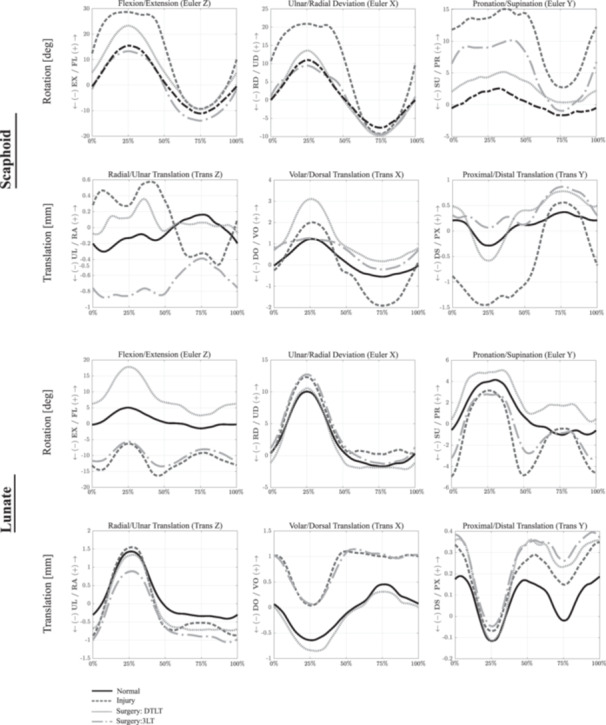
The objective of this study was to evaluate scaphoid, lunate and capitate kinematics after disruption to the primary and secondary scapholunate ligamentous stabilizers, and to assess the effectiveness of scapholunate ligament reconstruction in restoring carpal kinematics post-operatively. Seven upper extremities were harvested, and the scapholunate interosseous ligament (SLIL) was divided. Specimens were mounted onto a computer-controlled dynamic wrist simulator, and simulations of flexion-extension, radial-ulnar deviation, and dart-thrower's motion were undertaken by simulated force application to the wrist tendons. Three-dimensional kinematics of the scaphoid, lunate and capitate were measured using bi-plane X-ray fluoroscopy in the native and ligament deficient state. The SLIL was then reconstructed by either dorsal transarticular loop tenodesis (DTLT), or by the three-ligament tenodesis (3LT) technique, and re-evaluated. SLIL deficiency resulted in significant differences in carpal kinematics compared to that in the healthy wrist across all wrist motions (p < 0.05). The DTLT procedure corrected increased scaphoid ulnar deviation and pronation in the SLIL deficient wrist, but did not significantly improve scaphoid flexion or volar translation of the scaphoid. The 3LT reconstructive technique restored scaphoid flexion and ulnar deviation but did not correct pronation, the increased lunate extension, nor the volar and ulnar translation observed in the ligament deficient wrist. Three-dimensional scaphoid, lunate and capitate motion depends on SLIL integrity, with tears to this ligament resulting in pathological kinematics, which may be partially mitigated with DTLT and 3LT surgical reconstruction. These findings suggest that this surgical reconstruction of the SLIL may not mitigate long-term degenerative joint conditions at the wrist.
Keywords: carpal; kinematic model; scapholunate instability; scapholunate interosseous ligament; stereophotogrammetric analysis.
© 2025 The Author(s). Journal of Orthopaedic Research® published by Wiley Periodicals LLC on behalf of Orthopaedic Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Kitay A. and Wolfe S. W., “Scapholunate Instability: Current Concepts in Diagnosis and Management,” Journal of Hand Surgery 37, no. 10 (2012): 2175–2196. - PubMed
-
- Jones W. A., “Beware the Sprained Wrist. The Incidence and Diagnosis of Scapholunate Instability,” Journal of Bone and Joint Surgery British Volume 7–B, no. 2 (1988): 293–297. - PubMed
-
- Watson H. K. and Ballet F. L., “The SLAC Wrist: Scapholunate Advanced Collapse Pattern of Degenerative Arthritis,” Journal of Hand Surgery 9, no. 3 (1984): 358–365. - PubMed
-
- Kleinman W. B., Steichen J. B., and Strickland J. W., “Management of Chronic Rotary Subluxation of the Scaphoid by Scapho‐Trapezio‐Trapezoid Arthrodesis,” Journal of Hand Surgery 7, no. 2 (1982): 125–136. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
