

Disulfidptosis-related immune patterns predict prognosis and characterize the tumor microenvironment in oral squamous cell carcinoma
- PMID: 39894803
- PMCID: PMC11789412
- DOI: 10.1186/s12903-024-05279-2
Disulfidptosis-related immune patterns predict prognosis and characterize the tumor microenvironment in oral squamous cell carcinoma
Abstract
Background: Establishing a prognostic risk model based on immunological and disulfidptosis signatures enables precise prognosis prediction of oral squamous cell carcinoma (OSCC).
Methods: Differentially expressed immune and disulfidptosis genes were identified in OSCC and normal tissues. We examined the model's clinical applicability and its relationship to immune cell infiltration. Additionally, the risk score, ssGSEA, ESTIMATE, and CIBERSORT were used to evaluate the intrinsic molecular subtypes, immunological checkpoints, abundances of tumor-infiltrating immune cell types and proportions between the two risk groups. GO-KEGG and GSVA analyses were performed to identify enriched pathways.
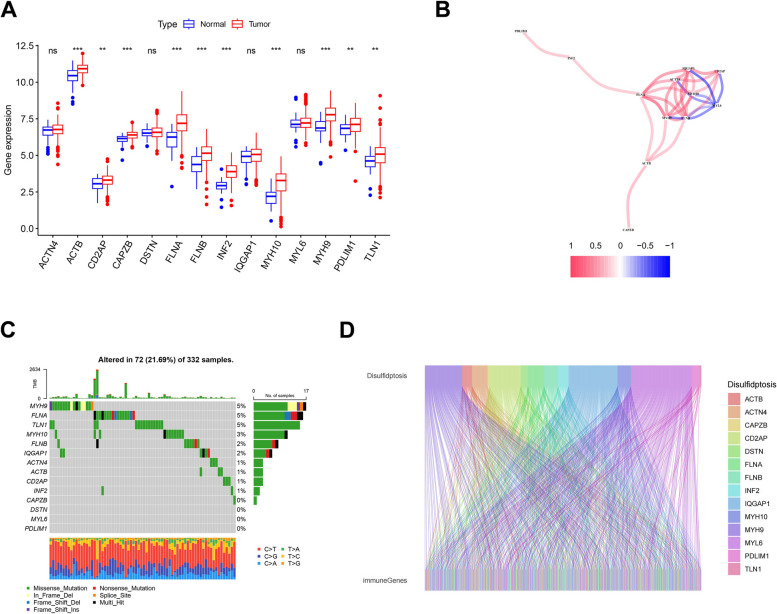
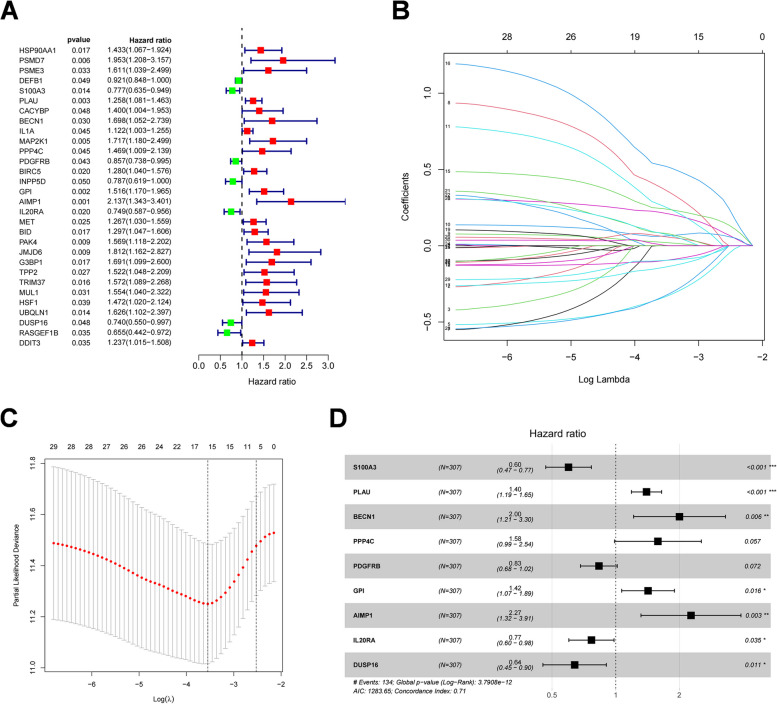
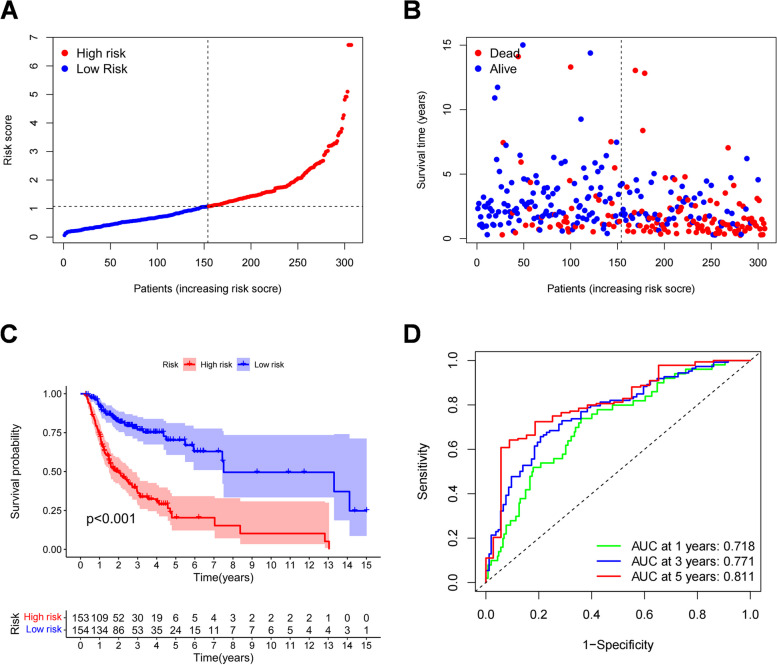
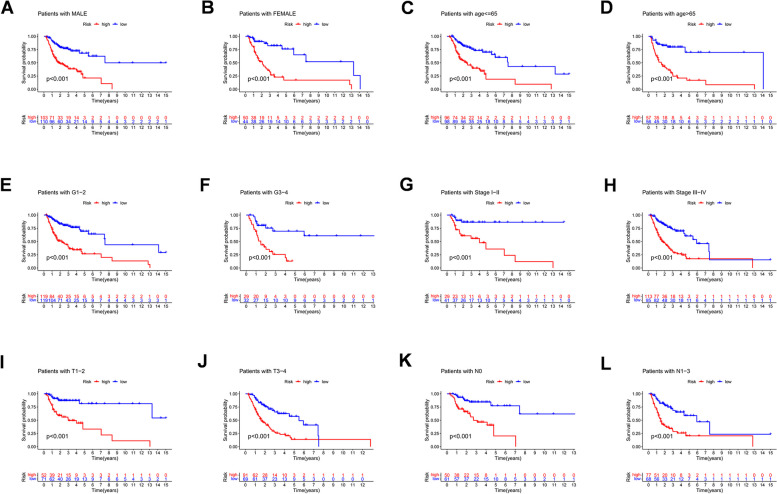
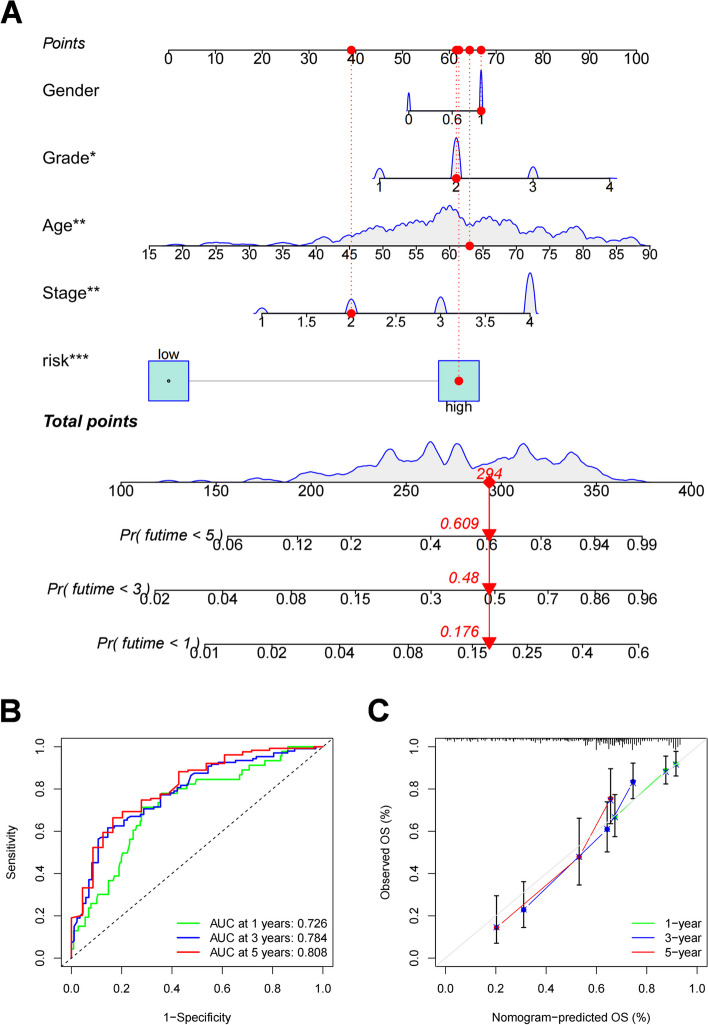
Results: We analyzed the correlation immune genes based on the 14 disulfidptosis-related genes, and found 379 disulfidptosis-related immune genes (DRIGs). After univariate Cox regression we obtained 30 DRIGs and least absolute shrinkage and selection operator (LASSO) regression to reduce the number of genes to 16. Finally we created a nine-DRIGs risk model, of which four were upregulated and five were downregulated. The analysis results showed that disulfidptosis was tightly related to immune cells, immunological-related pathways, the tumor microenvironment (TME), immune checkpoints, human leukocyte antigen (HLA), and tumor mutational burden (TMB). The nomogram, integrating the risk score and clinical factors, accurately predicted overall survival.
Conclusions: This novel risk model highlights the role of disulfidptosis-related immune genes in OSCC prognosis. With this model, we can more accurately predict the prognosis of patients with OSCC, as well as assess the potential effects of their TME and immunotherapy.
Keywords: Disulfidptosis; Immune gene; Oral squamous cell carcinoma; Prognosis; Risk model; TCGA.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. No.2022095 K was approved by Zhongnan Hospital of Wuhan University Medical Ethics Committee. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
A novel disulfidptosis-related LncRNA prognostic risk model: predicts the prognosis, tumor microenvironment and drug sensitivity in esophageal squamous cell carcinoma.BMC Gastroenterol. 2024 Nov 27;24(1):437. doi: 10.1186/s12876-024-03530-2. BMC Gastroenterol. 2024. PMID: 39604874 Free PMC article.
-
Disulfidptosis related immune genes drive prognostic model development and tumor microenvironment characterization in bladder urothelial carcinoma.Sci Rep. 2025 Mar 8;15(1):8130. doi: 10.1038/s41598-025-92297-x. Sci Rep. 2025. PMID: 40057601 Free PMC article.
-
Development and validation of a novel disulfidptosis-related lncRNAs signature in patients with HPV-negative oral squamous cell carcinoma.Sci Rep. 2024 Jun 23;14(1):14436. doi: 10.1038/s41598-024-65194-y. Sci Rep. 2024. PMID: 38910181 Free PMC article.
-
Development and experimental verification of a prognosis model for disulfidptosis-associated genes in HNSCC.Medicine (Baltimore). 2024 Mar 22;103(12):e37308. doi: 10.1097/MD.0000000000037308. Medicine (Baltimore). 2024. PMID: 38518012 Free PMC article. Review.
-
Advances in the study of disulfidptosis in digestive tract tumors.Discov Oncol. 2025 Feb 15;16(1):186. doi: 10.1007/s12672-025-01875-y. Discov Oncol. 2025. PMID: 39954025 Free PMC article. Review.
Cited by
-
Therapeutic Targeting of Apoptosis, Autophagic Cell Death, Necroptosis, Pyroptosis, and Ferroptosis Pathways in Oral Squamous Cell Carcinoma: Molecular Mechanisms and Potential Strategies.Biomedicines. 2025 Jul 16;13(7):1745. doi: 10.3390/biomedicines13071745. Biomedicines. 2025. PMID: 40722814 Free PMC article. Review.
-
Construction and validation of a chemokine-related gene signature associated with prognosis, clinical significance, and immune microenvironment characteristics in cervical cancer.Discov Oncol. 2025 Jun 15;16(1):1114. doi: 10.1007/s12672-025-02973-7. Discov Oncol. 2025. PMID: 40517358 Free PMC article.
References
-
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45(4–5):309–16. - PubMed
-
- Miranda-Filho A, Bray F. Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol. 2020;102:104551. - PubMed
-
- Nocini R, Lippi G, Mattiuzzi C. Biological and epidemiologic updates on lip and oral cavity cancers. Ann Cancer Epidemiol. 2020:4. 10.21037/ace.2020.01.01.
-
- Chow LQM. Head and Neck Cancer. N Engl J Med. 2020;382(1):60–72. - PubMed
-
- Ng SW, Syamim Syed Mohd Sobri SN, Zain RB, Kallarakkal TG, Amtha R, Wiranata Wong FA, Rimal J, Durward C, Chea C, Jayasinghe RD et al. Barriers to early detection and management of oral cancer in the Asia Pacific region. J Health Services Res Policy. 2022;27(2):133–140. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
