

Clonal Hematopoiesis and Risk of Heart Failure After Autologous Hematopoietic Cell Transplantation for Lymphoma
- PMID: 39896122
- PMCID: PMC11782012
- DOI: 10.1016/j.jaccao.2024.10.006
Clonal Hematopoiesis and Risk of Heart Failure After Autologous Hematopoietic Cell Transplantation for Lymphoma
Abstract
Background: Patients with lymphoma are at high risk for developing heart failure (HF) after autologous hematopoietic cell transplantation (HCT). More accurate risk determination pre-HCT may facilitate screening and prevention of HF.
Objectives: The aim of this study was to examine the association between clonal hematopoiesis of indeterminate potential (CHIP) and the risk for HF after HCT for lymphoma.
Methods: This was a retrospective cohort study of 861 patients who underwent autologous HCT for lymphoma between 2010 and 2016 at City of Hope Comprehensive Cancer Center. Targeted DNA sequencing was performed to determine the presence of CHIP (variant allele frequency ≥ 2%). The primary outcome of interest was the 5-year cumulative incidence of de novo HF. Other outcomes of interest included overall and cause-specific mortality.
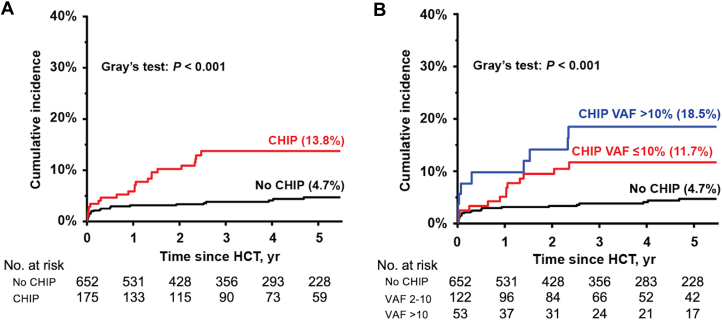
Results: Overall, 186 patients (21.7% of the cohort) had at least 1 CHIP variant, and 59 (6.9%) had ≥2 variants. DNMT3A, PPM1D, and TET2 were the most frequently mutated genes. The 5-year incidence of HF was significantly higher in patients with CHIP compared with those without CHIP (13.8% vs 4.7%; P < 0.001; sub-distribution hazard ratio [sHR]: 2.48; 95% CI: 1.32-4.68); the HF incidence increased by variant allele frequency: 0-2% (4.7%), 2-10% (11.7%), and >10% (18.5%), P < 0.001. Patients with CHIP had significantly worse overall survival after HCT, compared with those without (63.4% vs 80.3%; P < 0.001), due primarily to the higher risk for nonrelapse mortality (subdistribution HR: 5.37; 95% CI: 2.34-12.35).
Conclusions: CHIP was highly prevalent and associated with risk for HF and nonrelapse mortality after HCT. These findings highlight the role of CHIP as a novel biomarker and potential target for intervention to improve outcomes after autologous HCT.
Keywords: CHIP; autologous hematopoietic cell transplantation; biomarkers; heart failure; lymphoma; nonrelapse mortality.
© 2025 The Authors.
Conflict of interest statement
This work was supported by the V Foundation for Cancer Research (grant DT2019-006 to Dr Armenian). Drs Rhee and Armenian have received a research grant from Pfizer (unrelated to the present work). Dr Jamal has received research grants from Pfizer and Janssen (unrelated to the present work). Dr Natarajan has received grants from Allelica, Amgen, Apple, Boston Scientific, Genentech, and Novartis; is a consultant to Allelica, Apple, AstraZeneca, Blackstone Life Sciences, Foresite Labs, HeartFlow, Novartis, Genentech, and GV; is a scientific advisory board member for Esperion Therapeutics, Preciseli, and TenSixteen Bio; and is a scientific cofounder of TenSixteen Bio; and his spouse is an employee of Vertex Pharmaceuticals (all unrelated to the present work). Dr Herrera has received consultancy and research funding from AstraZeneca, ADC Therapeutics, Genentech, Bristol Myers Squibb, Seagen, and Merck; has received consultancy fees from Tubulis, Takeda, and Karyopharm; and has received research funding from Kite, a Gilead Company, and Gilead Sciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
