

The Cross-Sectional Areas and Anterior-Posterior Balance of the Cervical Paraspinal Muscles in Dropped Head Syndrome and Cervical Spondylotic Myelopathy: A Propensity Score-Matched Analysis
- PMID: 39896130
- PMCID: PMC11782067
- DOI: 10.1002/jsp2.70047
The Cross-Sectional Areas and Anterior-Posterior Balance of the Cervical Paraspinal Muscles in Dropped Head Syndrome and Cervical Spondylotic Myelopathy: A Propensity Score-Matched Analysis
Abstract
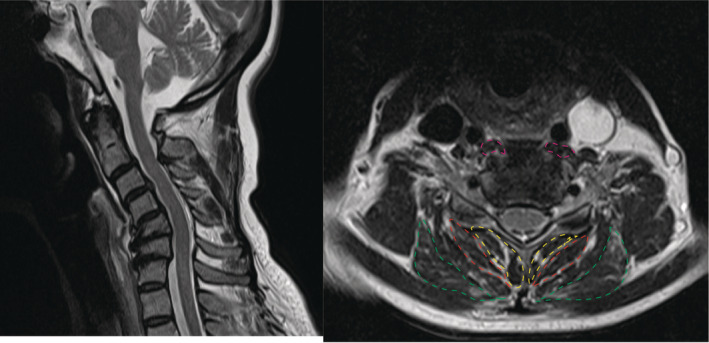
Introduction: Dropped head syndrome (DHS) is characterized by weakness of the neck extensor muscles. However, few studies have assessed the cross-sectional areas (CSAs) of the cervical paraspinal muscles (CPM) and their anterior-posterior balance in DHS. This study aimed to elucidate the pathognomonic findings of DHS by comparing the CSAs and anterior-posterior balance of the CPM in patients with DHS and cervical spondylotic myelopathy (CSM), using magnetic resonance imaging (MRI).
Methods: We compared the CSAs and anterior-posterior balance of the CPM in patients with DHS and CSM using MRI. Patients with CSM were selected in an age- and sex-matched manner, using the propensity score. The longus colli (LC) muscle was selected as the anterior muscle; and the semispinalis cervicis (SSC), splenius capitis (SC), and multifidus muscles (MM) were selected as the posterior muscles. We calculated LC/SSC, LC/SC, LC/MM, and LC/(SSC + SC + MM), as indicators of neck muscle balance.
Results: The DHS and the CSM cohort comprised 26 and 52 patients, respectively. Both cohorts had a mean age of 71-year-old. There were no significant differences in the CSAs and most of the indicators of neck balance between the two cohorts. However, the LC/SSC was significantly higher in the DHS cohort than that in the CSM cohort (40.3% and 29.1%, respectively; p < 0.01).
Conclusions: Our study highlights a unique anterior-posterior imbalance in the CPM of DHS patients, differing from CSM patients. Strengthening the SSC muscle could be a key to preventing DHS progression.
Keywords: Dropped head syndrome; anterior–posterior muscle balance; longus colli muscle; semispinalis cervicis muscle.
© 2025 The Author(s). JOR Spine published by Wiley Periodicals LLC on behalf of Orthopaedic Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Suarez G. A. and J. J. Kelly, Jr. , “The Dropped Head Syndrome,” Neurology 42 (1992): 1625–1627. - PubMed
-
- Katz J. S., Wolfe G. I., Burns D. K., et al., “Isolated Neck Extensor Myopathy: A Common Cause of Dropped Head Syndrome,” Neurology 46 (1996): 917–921. - PubMed
-
- Kastrup A., Gdynia H. J., Nägele T., and Riecker A., “Dropped‐Head Syndrome due to Steroid Responsive Focal Myositis: A Case Report and Review of the Literature,” Journal of the Neurological Sciences 267 (2008): 162–165. - PubMed
-
- Kashihara K., Ohno M., and Tomita S., “Dropped Head Syndrome in Parkinson's Disease,” Movement Disorders 21 (2006): 1213–1216. - PubMed
