

Features of myositis and myasthenia gravis in patients treated with immune checkpoint inhibitors: a multicentric, retrospective cohort study
- PMID: 39896961
- PMCID: PMC11782875
- DOI: 10.1016/j.lanepe.2024.101192
Features of myositis and myasthenia gravis in patients treated with immune checkpoint inhibitors: a multicentric, retrospective cohort study
Abstract
Background: Immune checkpoint inhibitors (ICIs) may induce overlapping myositis/myasthenia gravis (MG) features, sparking current debate about pathophysiology and management of this emerging disease entity. We aimed to clarify whether ICI-induced (ir-) myositis and ir-MG represent distinct diseases or exist concurrently.
Methods: We performed a retrospective multicenter cohort study. Using the Paris University Hospitals database (n = 2,910,417), we screened all patients with International Classification of Diseases codes or free text related to myositis/MG signs and ICI (n = 620). 'Ir-MG signs' were defined by fatigability, repetitive nerve stimulation (RNS) decrement, and/or acetylcholine receptor antibodies (AChR Abs).
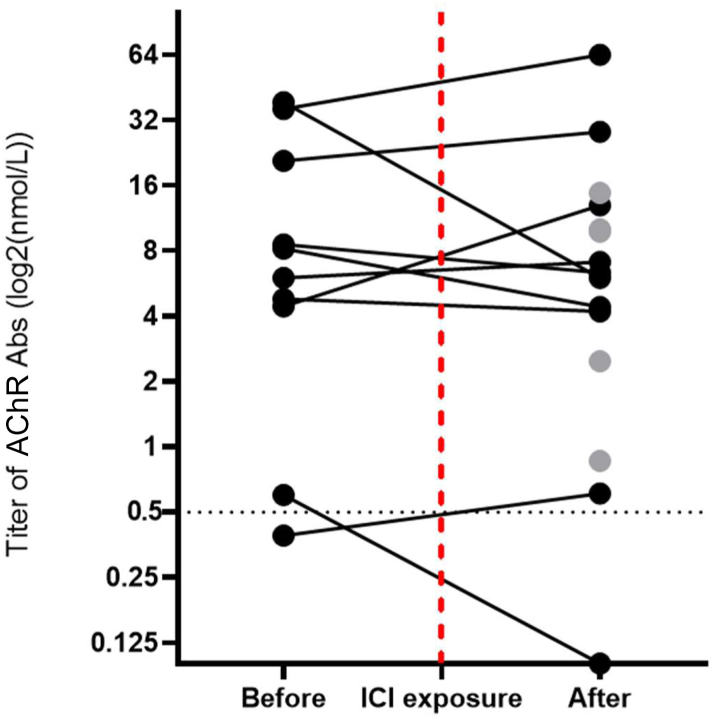
Findings: Ir-MG signs were never observed in the absence of ir-myositis (pathological diagnosis (n = 12/14) or CK levels >8000 U/L (n = 2/14)). Among ir-myositis patients, fatigability (2%; n = 1/62) and RNS decrement (2%; n = 1/41) were demonstrated only in one patient with pre-existing MG. AChR Abs testing yielded positive results in 26% of ir-myositis patients (n = 14/53). We revealed that test results were already positive prior to ICI therapy (n = 8/9). Clinically, ir-myositis frequently presented with "MG-like" oculomotor disease (50%; n = 31/62), bulbar dysfunction affecting speech (29%; n = 18/62) and swallowing (42%; n = 26/62), and respiratory disorders (53%; n = 33/62). Extraocular and diaphragm muscles necropsies disclosed intense muscle inflammation (100%; n = 5/5).
Interpretation: In our extensive database, we found no evidence of isolated ir-MG, nor of clear neuromuscular junction dysfunction in ir-myositis. These findings suggest that patients with ir-MG suspicion frequently have ir-myositis and ir-MG might be rare. "MG-like" symptoms may stem from ir-myositis-specific predilection for oculo-bulbo-respiratory musculature. Indeed, we revealed florid inflammatory infiltration of the oculomotor and respiratory muscles. Additional studies are needed to confirm these results and to elucidate the role of pre-existing AChR Abs in ir-myositis.
Funding: None.
Keywords: Acetylcholine receptor antibodies; Autoimmunity; Biomarker; Immune checkpoint inhibitor; Immune checkpoint inhibitor-induced myasthenia gravis; Immune checkpoint inhibitor-induced myositis; Immune-related adverse event; Immunotherapy; Myasthenia gravis; Myositis.
© 2025 The Authors.
Conflict of interest statement
None of the authors received financial support for the submitted work. CA reports one patent planned in the field of management of immune checkpoint inhibitors toxicities. BA reports a research grant from MSD Avenir, consulting fees from Novartis, Astellas, and Sanofi, personal honorarium from Sanofi, AstraZeneca, BMS, MSD and Astellas, and support for attending meetings and/or travel from Janssen, MSD, Pfizer, IPSEN Pharma and Takeda. MT reports a grant from Sanofi, consulting fees from Servier, Novocure and NH TherAguiX, personal honorarium from Servier, Novocure and ONO, and support for attending meetings and/or travel from Servier. MT participated on a Data Safety Monitoring or Advisory Board for Servier. MCB reports personal honorarium, and support for attending meetings and/or travel from Novartis. SE reports consulting fees from Bayer, Amgen and Ipsen, and personal honorarium from AstraZeneca, BMS, Philips, General Electric, and Eisai. FT reports non-personal consulting fees from MSD, Novartis, and GSK. JES reports personal consulting fees from AstraZeneca, BeiGene, BMS and Novartis, several patents planned, issued or pending in the field of management of immune checkpoint inhibitors toxicities. YA received research funding from Sanofi and Association Recherche contre le Cancer, consulting fees from BMS, personal honorarium from RE-IMAGINE Health Agency and CSL Behring SA, and support for attending meetings and/or travel from CSL Behring SA and Boehringer Ingelheim France. YA had several patents planned, issued or pending in the field of management of immune checkpoint inhibitors toxicities.
Figures



References
-
- Wing K., Onishi Y., Prieto-Martin P., et al. CTLA-4 control over Foxp3+ regulatory T cell function. Science. 2008;322(5899):271–275. - PubMed
-
- Waterhouse P., Penninger J.M., Timms E., et al. Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science. 1995;270(5238):985–988. - PubMed
-
- Nishimura H., Nose M., Hiai H., Minato N., Honjo T. Development of lupus-like autoimmune diseases by disruption of the PD-1 gene encoding an ITIM motif-carrying immunoreceptor. Immunity. 1999;11(2):141–151. - PubMed
-
- Dong H., Strome S.E., Salomao D.R., et al. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med. 2002;8(8):793–800. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
