

Hemorrhagic Pericardial Effusion Secondary to Coxsackie B Pericarditis
- PMID: 39897235
- PMCID: PMC11787821
- DOI: 10.7759/cureus.76861
Hemorrhagic Pericardial Effusion Secondary to Coxsackie B Pericarditis
Abstract
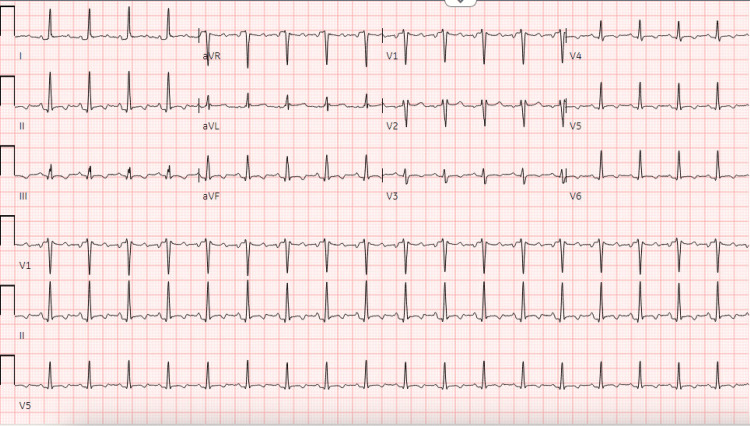
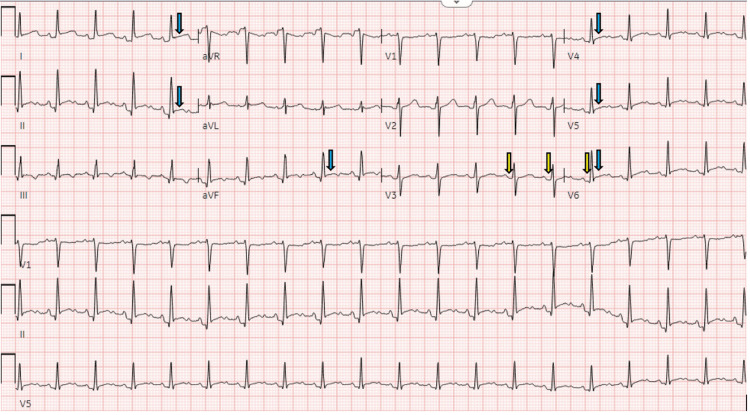
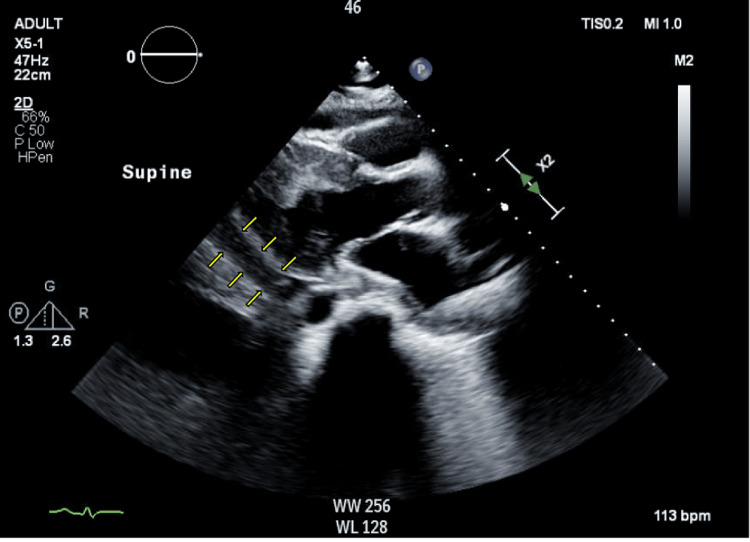
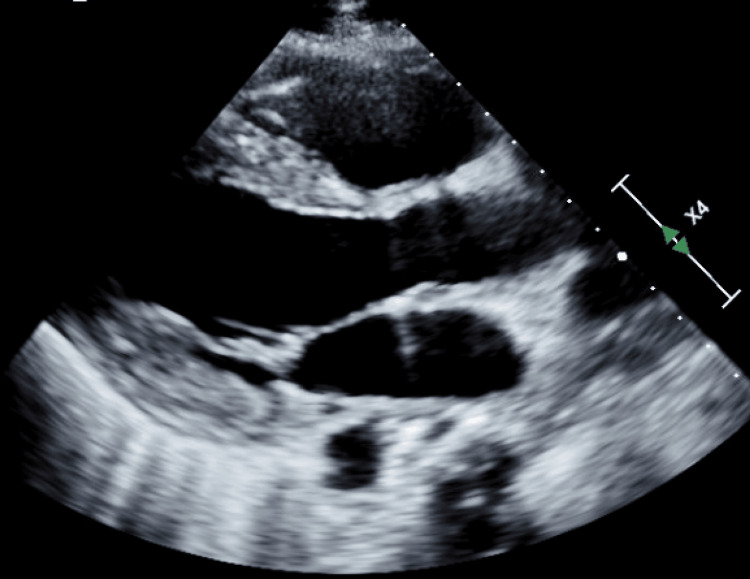
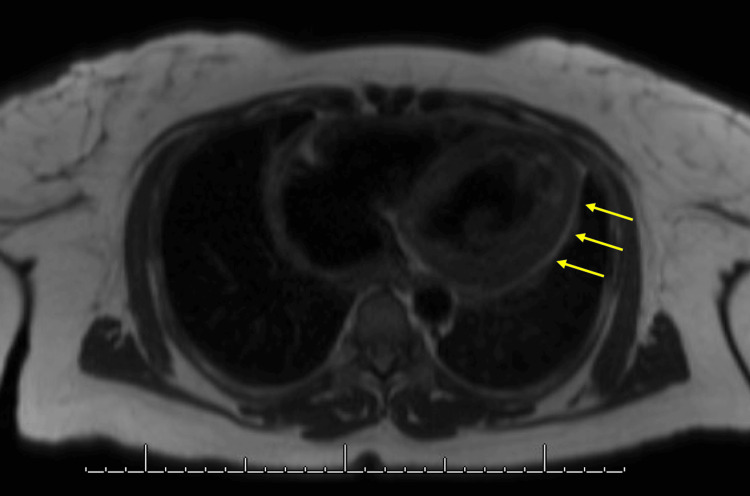
Acute pericarditis is caused by inflammation of the pericardial sac. Among the vast number of potential causes, viruses tend to trigger pericarditis most frequently. Some of the more common viral causes are Coxsackie A/B, echovirus, adenovirus, cytomegalovirus, herpes simplex virus, and human immunodeficiency virus. Pericardial effusion is a common complication and can be visualized on echocardiogram. In some cases, the pericardial effusion can be hemorrhagic in nature, which is extremely rare in the setting of viral pericarditis. The most common causes of hemorrhagic effusion are myocardial infarction, trauma, aortic dissection, or coronary artery bypass graft surgery. Pericardial effusion can sometimes result in serious complications such as cardiac tamponade. In cases of significant pericardial effusion, pericardiocentesis may be required. We present an interesting case of pericarditis caused by the Coxsackie B virus, causing significant hemorrhagic pericardial effusion requiring pericardiocentesis in a young patient. A 37-year-old female with no relevant past medical history presented with substernal chest pain radiating to the left arm and shoulder that improved with leaning forward and dyspnea for two weeks. She had a two-week history of a cough, dysphagia, fever, and chills that started two days prior to the presentation. EKG showed widespread ST elevations and PR interval depressions, which is consistent with a diagnosis of pericarditis. A large pericardial effusion was present on echocardiogram, further suggesting possible pericarditis. Around 350 mL of fluid was removed by pericardiocentesis. Cell count showed 201,000 red blood cells (RBCs)/mcL and 9,350 nucleated cells/mcL. Cytology was negative for malignancy. Cultures were negative for bacteria and fungi. Serum serology showed elevated inflammatory markers (C-reactive protein of 140 mg/L and erythrocyte sedimentation rate of 112 mm/hr) and increased Coxsackie B antibody titers (1:160 for type 2 and 1:320 for type 3). She was started on non-steroidal anti-inflammatory drugs and colchicine. This is a unique case showing that while small exudative pericardial effusions may occur with viral pericarditis, viral infections can also cause a significant hemorrhagic pericardial effusion. Most Coxsackie virus infections are benign. However, there are a few documented case reports of hemorrhagic pericardial effusion from Coxsackie B causing tamponade and death. The importance of this case is that it highlights the consideration of viral infections such as Coxsackie B as a potential cause of hemorrhagic tamponade, especially during autumn and winter months, seasons with the highest risk.
Keywords: coxsackie b; echocardiogram; hemorrhagic pericardial effusion; pericarditis; viral pericarditis.
Copyright © 2025, Shoukri et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Coxsackie B viral infection presenting with hemorrhagic pericardial effusion and pleural effusion.Ann Pediatr Cardiol. 2022 Jan-Feb;15(1):87-89. doi: 10.4103/apc.apc_21_21. Epub 2022 Jun 14. Ann Pediatr Cardiol. 2022. PMID: 35847405 Free PMC article.
-
Takotsubo cardiomyopathy complicated by cardiac tamponade due to non-hemorrhagic pericardial effusion: a case report.BMC Cardiovasc Disord. 2020 Feb 6;20(1):67. doi: 10.1186/s12872-020-01377-5. BMC Cardiovasc Disord. 2020. PMID: 32028901 Free PMC article.
-
[Recurrent autoreactive pericardial effusion. Impact of an aetiological classification of pericarditis].Dtsch Med Wochenschr. 2006 Sep 29;131(39):2143-6. doi: 10.1055/s-2006-951342. Dtsch Med Wochenschr. 2006. PMID: 16991029 German.
-
[Toxoplasma pericarditis without immunosuppressant disorder detected by polymerase chain reaction of pericardial fluid: a case report].J Cardiol. 2000 Jan;35(1):47-54. J Cardiol. 2000. PMID: 10654250 Review. Japanese.
-
Management strategies in pericardial emergencies.Herz. 2006 Dec;31(9):891-900. doi: 10.1007/s00059-006-2937-0. Herz. 2006. PMID: 17180653 Review.
References
-
- Pericarditis. Troughton RW, Asher CR, Klein AL. Lancet. 2004;363:717–727. - PubMed
-
- 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS) Adler Y, Charron P, Imazio M, et al. Eur Heart J. 2015;36:2921–2964. - PMC - PubMed
-
- Evaluation and treatment of pericarditis: a systematic review. [ Nov; 2023 ];Imazio M, Gaita F, LeWinter M. JAMA. 2015 314:1498–1506. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous