

Which muscle is the external rotation compensator after superior capsular reconstruction?
- PMID: 39898197
- PMCID: PMC11784471
- DOI: 10.1016/j.jseint.2024.09.010
Which muscle is the external rotation compensator after superior capsular reconstruction?
Abstract
Background: Superior capsular reconstruction (SCR) is a surgical option for massive irreparable rotator cuff tears, particularly involving the supraspinatus and infraspinatus. In this procedure, the torn infraspinatus is not repaired or reconstructed. However, an improvement in postoperative external rotation (ER) angle and strength is observed. There is a lack of studies explaining how ER is restored after SCR. The aim of this study is to identify the ER compensator by assessing the muscle volume of the posterior deltoid and teres minor.
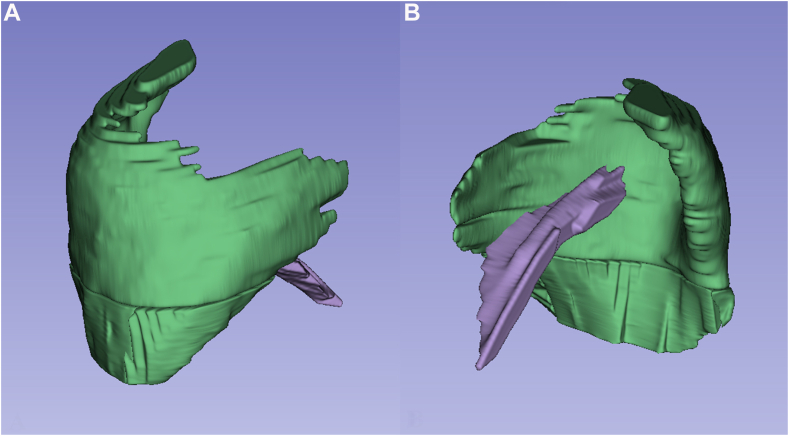
Methods: Sixty-eight patients with massive rotator cuff tears underwent SCR during 2016-2021. Of these patients, 28 who met the following inclusion criteria were retrospectively reviewed: (1) massive rotator cuff tears, including the supraspinatus and infraspinatus, (2) severe muscle atrophy and fatty change, (3) intact or reparable subscapularis tendon, and (4) Hamada of grade 3 or lower. Posterior deltoid and teres minor volume were measured using open-source medical image processing software preoperatively and 1-year postoperatively. The percentage of the posterior deltoid and teres minor muscle volume change was compared between patients with 1-year postoperative ER manual muscle testing (MMT) of grade 5 and of grade < 5. The relationship between grade of fatty change, percentage of the muscle volume change, and ER angle and strength were evaluated.
Results: There was a significant increase in the 1-year postoperative teres minor volume compared with the preoperative volume (24.6 ± 10.3 cm³ vs. 20.9 ± 8.3 cm³, P < .000), while the posterior deltoid volume remained unchanged (178.1 ± 48.3 cm³ vs. 178.8 ± 47 cm³). Patients with ER MMT of grade 5 had a greater teres minor volume change compared to those with an ER MMT grade of less than 5 (22.3% vs. 9.4%), although this difference was not significant (P = .074, 95% CI = -1.3 to 27.0). The posterior deltoid volume showed no significant change. The percentage of teres minor volume change had a weak positive correlation with ER strength (r = 0.308, P = .055, 95% CI = -0.02 to 1.0). There was a significant negative correlation between ER strength and the severity of both preoperative and postoperative fatty changes in the teres minor (r = -0.258, P = .065, 95% CI = -1.0 to -0.042 and r = -0.323, P = .028, 95% CI = -1.0 to -0.113, respectively). The pre and postoperative fatty changes in the teres minor were negatively correlated with the percentage of teres minor volume change (r = -0.298, P = .062, 95% CI = -1.0 to 0.031 and r = -0.413, P = .015, 95% CI = -1.0 to -0.1, respectively).
Conclusion: The teres minor may serve as a potential compensator for ER in patients with massive rotator cuff tears following SCR.
Keywords: External rotation compensator; Massive irreparable rotator cuff tear; Muscle volume study; Posterior deltoid; Superior capsular reconstruction; Teres minor.
© 2024 The Author(s).
Figures

Similar articles
-
Combined Anterior Latissimus Dorsi and Teres Major Tendon Transfer (aLDTM) for Irreparable Anterosuperior Rotator Cuff Tears.JBJS Essent Surg Tech. 2024 Apr 19;14(2):e23.00060. doi: 10.2106/JBJS.ST.23.00060. eCollection 2024 Apr-Jun. JBJS Essent Surg Tech. 2024. PMID: 38645756 Free PMC article.
-
Results of latissimus dorsi tendon transfer for irreparable cuff tears.Orthop Traumatol Surg Res. 2009 Apr;95(2):108-13. doi: 10.1016/j.otsr.2008.10.002. Epub 2009 Apr 5. Orthop Traumatol Surg Res. 2009. PMID: 19349223
-
A Biomechanical Analysis of Shoulder Muscle Excursions During Abduction, After the Treatment of Massive Irreparable Rotator Cuff Tears Using Superior Capsular Reconstruction (SCR), Bursal Acromial Reconstruction (BAR), and SCR with BAR.J Shoulder Elb Arthroplast. 2022 Jun 23;6:24715492221109001. doi: 10.1177/24715492221109001. eCollection 2022. J Shoulder Elb Arthroplast. 2022. PMID: 35782774 Free PMC article.
-
Lower Trapezius Transfer for Irreparable Posterosuperior Rotator Cuff Tears.Curr Rev Musculoskelet Med. 2024 Apr;17(4):93-100. doi: 10.1007/s12178-024-09885-z. Epub 2024 Jan 31. Curr Rev Musculoskelet Med. 2024. PMID: 38294674 Free PMC article. Review.
-
Lower trapezius transfer for massive posterosuperior rotator cuff defects.Oper Orthop Traumatol. 2022 Feb;34(1):34-44. doi: 10.1007/s00064-021-00756-1. Epub 2021 Dec 16. Oper Orthop Traumatol. 2022. PMID: 34918172 Review. English.
References
-
- Azevedo C.I.C., Catarina Leiria Pires Gago Ângelo A., Campos-Correia D., Delgado L., Ferreira N., Sevivas N. Clinical importance of graft integrity in arthroscopic superior capsular reconstruction using a minimally invasively harvested midthigh fascia lata autograft: 3-year clinical and magnetic resonance imaging outcomes. Am J Sports Med. 2020;48:2115–2128. doi: 10.1177/0363546520928649. - DOI - PubMed
-
- Boileau P., McClelland W.B., Jr., Rumian A.P. Massive irreparable rotator cuff tears:how to rebalance the cuff-deficient shoulder. Instr Course Lect. 2014;63:71–83. - PubMed
-
- Boileau P., McClelland W.B., Jr., Rumian A.P. Massive irreparable rotator cuff tears: how to rebalance the cuff-deficient shoulder. Instr Course Lect. 2014;63:71–83. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous