

IDH-mutant astrocytomas with primitive neuronal component have a distinct methylation profile and a higher risk of leptomeningeal spread
- PMID: 39899075
- PMCID: PMC11790679
- DOI: 10.1007/s00401-025-02849-8
IDH-mutant astrocytomas with primitive neuronal component have a distinct methylation profile and a higher risk of leptomeningeal spread
Abstract
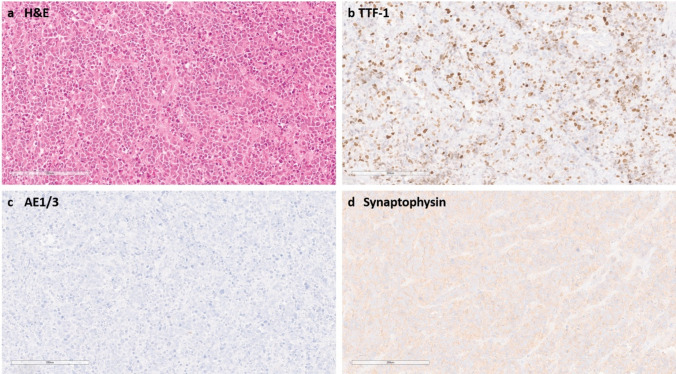
IDH-mutant astrocytomas are diffuse gliomas that are defined by characteristic mutations in IDH1 or IDH2 and do not have complete 1p/19q co-deletion. The established grading criteria include histological features of brisk mitotic activity (grade 3) and necrosis and/or microvascular proliferation (grade 4). In addition, homozygous deletion of the CDKN2A/B locus has recently been implemented as a molecular marker for grade 4 IDH-mutant astrocytomas. Here, we describe a subgroup of high-grade IDH-mutant astrocytomas characterised by a primitive neuronal component based on histology and a distinct DNA methylation profile (n = 51, ASTRO PNC). Misinterpretation as carcinoma metastasis was common, since GFAP expression was absent in the primitive neuronal component, whereas TTF-1 expression was detected in 15/19 cases (79%) based on immunohistochemistry. Apart from mutations in IDH1, TP53, and ATRX, we observed enrichment for alterations in RB1 (n = 19/51, 37%) and MYCN (n = 14/51, 27%). Homozygous CDKN2A/B deletion (n = 1/51, 2%) and CDK4 amplification (n = 3/51, 6%) were relatively rare events. Clinical (n = 31 patients) and survival data (n = 23 patients) indicate a clinical behaviour similar to other CNS WHO grade 4 IDH-mutant astrocytomas, however with an increased risk for leptomeningeal (n = 7) and extra-axial (n = 2) spread. Taken together, ASTRO PNC is defined by a distinct molecular and histological appearance that can mimic metastatic disease and typically follows an aggressive clinical course.
Keywords: MYCN; RB1; Astrocytoma; DNA methylation; IDH-mutant; Primitive neuronal component.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: MS is scientific advisor and shareholder of Heidelberg Epignostix and Halo Dx, and a scientific advisor of Arima Genomics, and InnoSIGN, and received research funding from Lilly USA, and Illumina USA. DC, SMP, DS, AvD and FS are shareholders of Heidelberg Epignostix. Ethical approval: Collection and analysis of corresponding tissue samples and clinical data was performed in accordance with local ethics regulations (local ethics vote S-318/2022) and in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Figures





References
-
- Banan R, Stichel D, Bleck A, Hong B, Lehmann U, Suwala A et al (2020) Infratentorial IDH-mutant astrocytoma is a distinct subtype. Acta Neuropathol 140:569–581. 10.1007/s00401-020-02194-y - PubMed
-
- Bingle CD (1997) Thyroid transcription factor-1. Int J Biochem Cell Biol 29:1471–1473. 10.1016/s1357-2725(97)00007-1 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
