

A prediction nomogram for residual after negative pressure aspiration for endogenic cesarean scar ectopic pregnancy: a retrospective study
- PMID: 39901095
- PMCID: PMC11789346
- DOI: 10.1186/s12884-025-07255-2
A prediction nomogram for residual after negative pressure aspiration for endogenic cesarean scar ectopic pregnancy: a retrospective study
Abstract
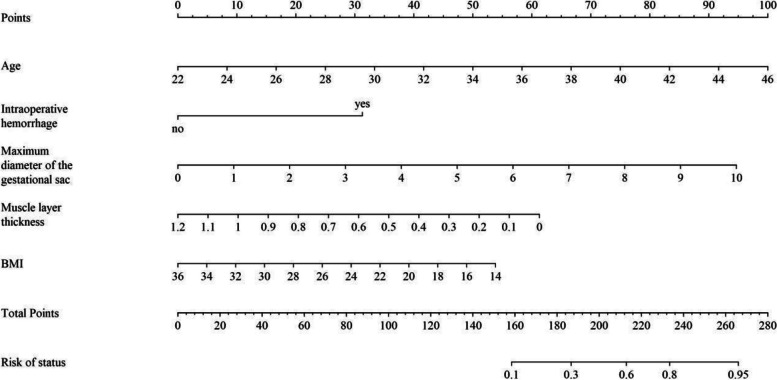
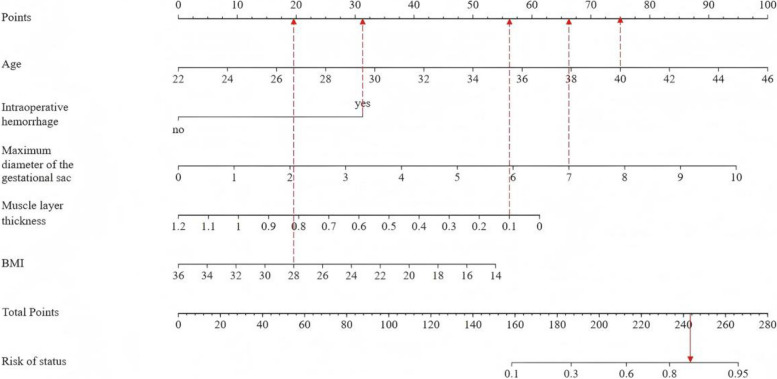
Background: We aimed to establish a predictive nomogram to evaluate the incidence of residual tissue in patients with endogenic cesarean scar ectopic pregnancy after negative pressure aspiration.
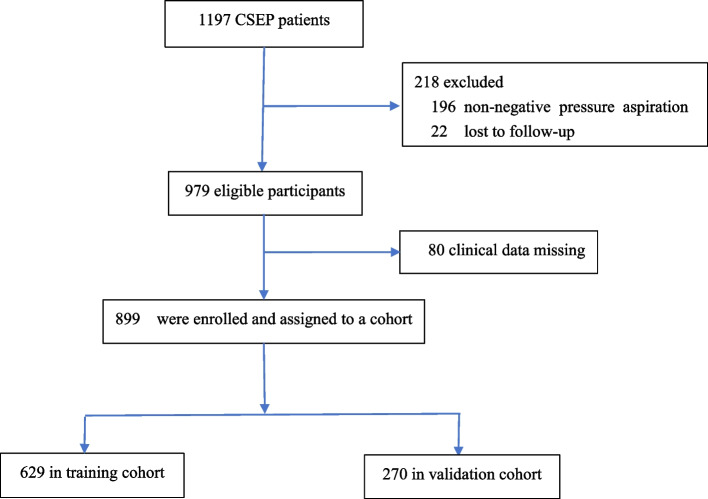
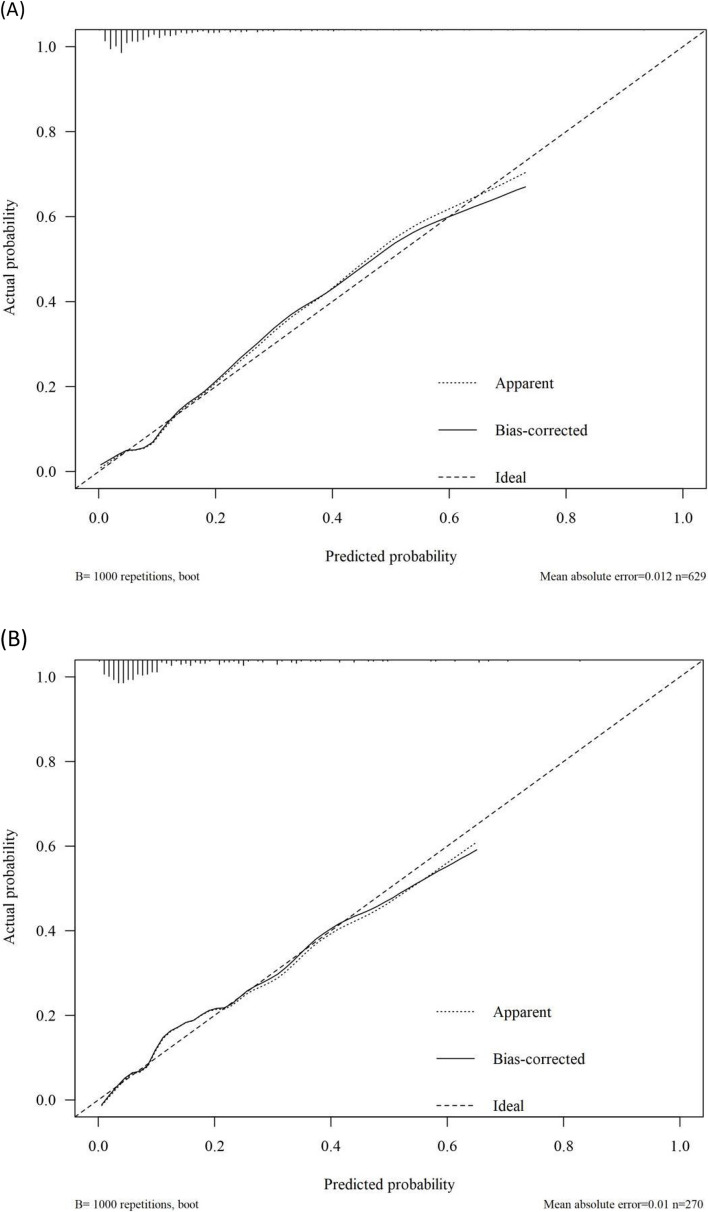
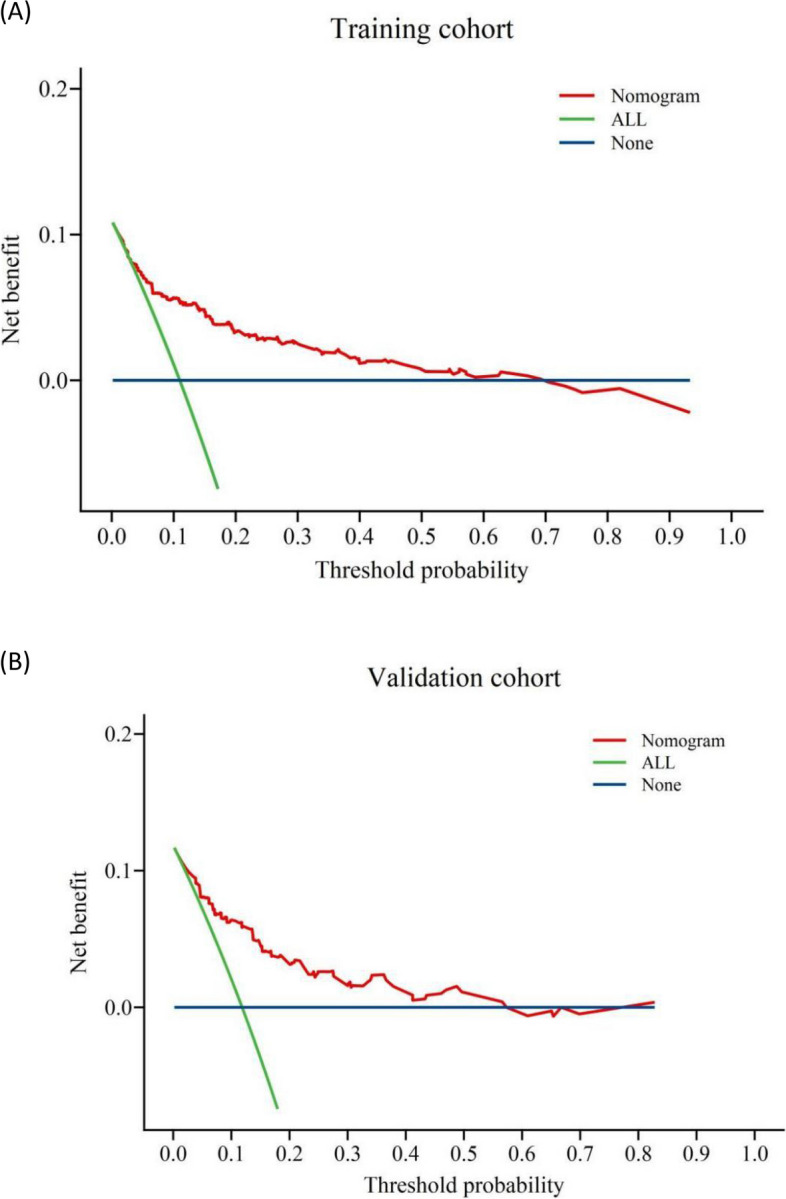
Methods: This retrospective study included patients treated in the gynecology department of our institution from May 2017 to August 2023 who underwent negative pressure suction treatment, ultrasound examinations before and after treatment, and received telephone follow-up for at least 6 months. A total of 899 patients met the inclusion criteria and were divided into a training cohort (629 patients, 70%) and a validation cohort (270 patients, 30%). Independent predictive factors were established using multivariate logistic regression. The resulting nomogram was validated using 1,000 bootstrap resampling, and calibration curves were plotted. Receiver operating characteristic (ROC) analysis was performed to calculate the area under the curve, sensitivity, specificity, and other metrics to assess its discriminative performance. Clinical decision curves were constructed to evaluate clinical applicability and quantify the net benefit within a range of threshold probabilities. The model was externally validated in the validation cohort.
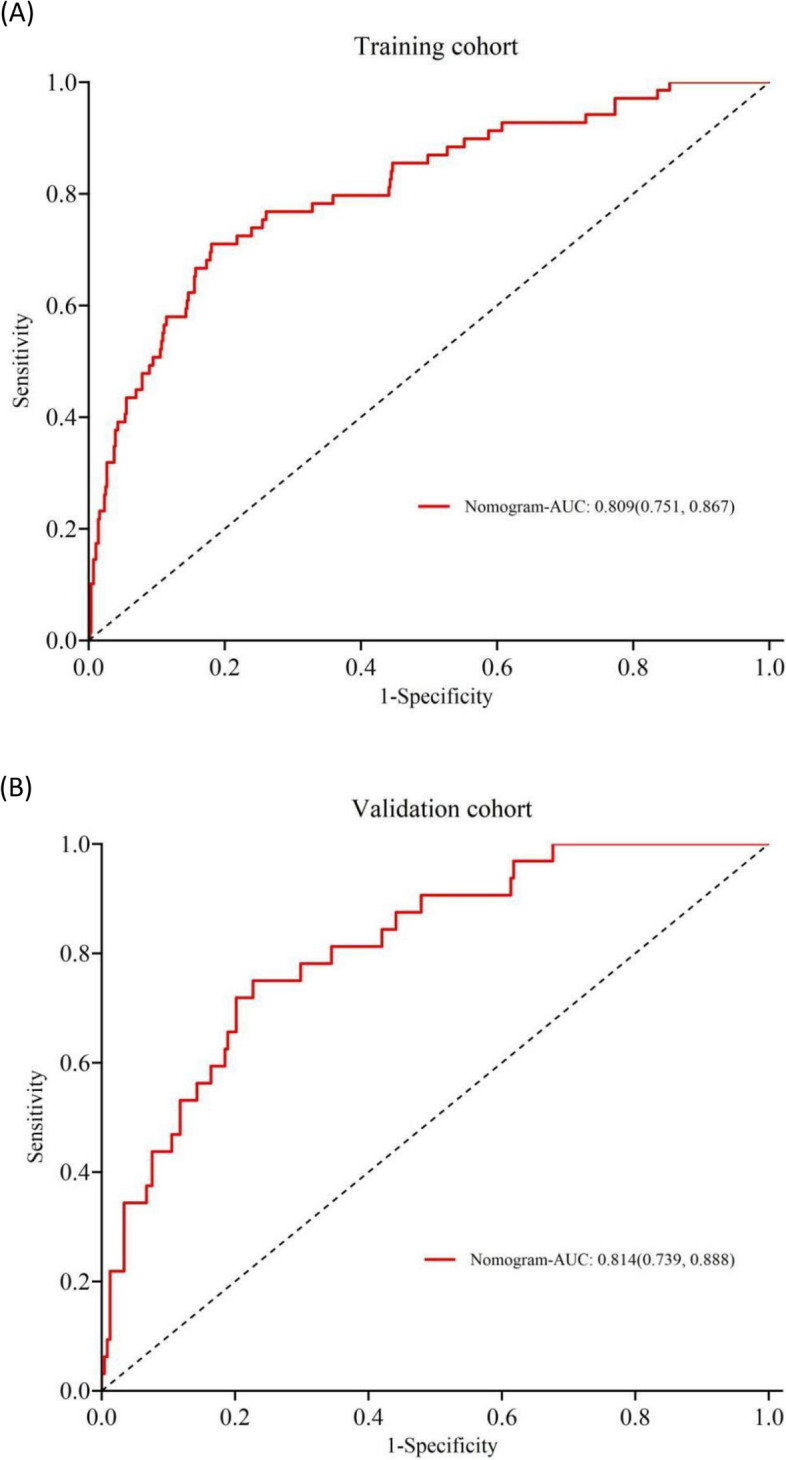
Results: Predictive factors included in the nomogram included age (hazard ratio [HR]: 1.220, 95% confidence interval [CI]: 1.135-1.316), BMI (HR: 0.890, 95% CI: 0.796-0.986), intraoperative major hemorrhage (HR: 4.457, 95% CI: 1.610-12.292), maximum diameter of the gestational sac (HR: 1.572, 95% CI: 1.295, 1.914), and thickness of the remaining muscle layer of the lower uterine segment (HR: 1.572, 95% CI: 0.014, 0.430). The ROC curve of the resulting nomogram showed similar area under the curve values for the training (0.809, 95% CI: 0.751-0.867) and validation cohorts (0.814, 95% CI: 0.739, 0.888). The Hosmer-Lemeshow test indicated good model fit (P = 0.861), and the calibration curve was close to the ideal diagonal line. Decision curve analysis demonstrated good net benefit, and external validation confirmed its reliability.
Conclusions: The model may aid in individual clinical decision-making, allowing clinicians to perform immediate postoperative assessments for patients with endogenous ectopic pregnancy in cesarean section scars treated with negative pressure suction, identify high-risk subpopulations, and select appropriate supplementary treatment in advance, making it particularly suitable for low-income areas and resource-limited primary hospitals.
Keywords: Cesarean scar ectopic pregnancy; Endogenic cesarean scar ectopic pregnancy; Prediction nomogram; Residual.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study involves human participants.Ethical clearance and support letters were obtained from the Ethical Committee with the reference number 2023IEC123 in November,2023.The methods were conducted following the tenets of the Helsinki declaration. Before collecting data, an information sheet was read to all eligible study participants to obtain oral informed consent. The privacy of the respondents was respected and data were deidentified before analysis and reported in aggregate. Participants gave informed consent to participate in the study before taking part. Consent for publication: We confirm that all authors have read and approved the final version of the manuscript and agree with its submission for publication. We also affirm that this manuscript has not been submitted to any other publication concurrently. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Predictive nomogram of ultrasound indicators for the termination outcome of caesarean scar pregnancy.Sci Rep. 2024 Dec 28;14(1):31378. doi: 10.1038/s41598-024-82894-7. Sci Rep. 2024. PMID: 39733108 Free PMC article.
-
Surgical treatment of Cesarean scar ectopic pregnancy: efficacy and safety of ultrasound-guided suction curettage.Ultrasound Obstet Gynecol. 2016 Apr;47(4):511-7. doi: 10.1002/uog.15857. Ultrasound Obstet Gynecol. 2016. PMID: 26764166
-
Cesarean Scar Ectopic Pregnancy Clinical Classification System With Recommended Surgical Strategy.Obstet Gynecol. 2023 May 1;141(5):927-936. doi: 10.1097/AOG.0000000000005113. Epub 2023 Apr 5. Obstet Gynecol. 2023. PMID: 37023450 Free PMC article.
-
Interventions for non-tubal ectopic pregnancy.Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD011174. doi: 10.1002/14651858.CD011174.pub2. Cochrane Database Syst Rev. 2020. PMID: 32609376 Free PMC article.
-
Treatment of viable cesarean scar ectopic pregnancy with suction curettage.Int J Gynaecol Obstet. 2005 May;89(2):163-6. doi: 10.1016/j.ijgo.2004.12.038. Int J Gynaecol Obstet. 2005. PMID: 15847889 Review.
References
-
- Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review. Am J Obstet Gynecol. 2012;207:14-29.10. - PubMed
-
- Birch Petersen K, Hoffmann E, Rifbjerg Larsen C, Svarre NH. Cesarean scar pregnancy: a systematic review of treatment studies. Fertil Steril. 2016;105:958–67. - PubMed
-
- Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies: etiology, diagnosis, and management. Obstet Gynecol. 2006;107(6):1373–81. - PubMed
-
- Gonzalez N, Tulandi T. Cesarean Scar Pregnancy: A Systematic Review. J Minim Invasive Gynecol. 2017;24(5):731–8. - PubMed
-
- Timor-Tritsch IE, Monteagudo A, Cali G, D’Antonio F, Kaelin Agten A. Cesarean scar pregnancy: diagnosis and pathogenesis. Obstet Gynecol Clin North Am. 2019;46:797–811. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
