

Role of 18F-PSMA-1007 PET/CT-derived quantitative volumetric tumor parameters in cytoreductive radical prostatectomy selection for patients with low-volume metastatic hormone-sensitive prostate cancer: a retrospective study
- PMID: 39901140
- PMCID: PMC11789373
- DOI: 10.1186/s12885-025-13482-9
Role of 18F-PSMA-1007 PET/CT-derived quantitative volumetric tumor parameters in cytoreductive radical prostatectomy selection for patients with low-volume metastatic hormone-sensitive prostate cancer: a retrospective study
Abstract
Background: Cytoreductive radical prostatectomy (cRP) has emerged as a promising therapeutic approach for low-volume metastatic hormone-sensitive prostate cancer (mHSPC), but the best candidates for cRP are still unknown. This study aims to explore the potential value of 18F-PSMA-1007 PET/CT-derived quantitative volumetric tumor parameters in cRP treatment selection among patients with low-volume mHSPC.
Methods: A total of 122 patients with primary low-volume mHSPC who underwent 18F-PSMA-1007 PET/CT followed by systemic therapy alone or plus cRP were included. The whole-body PSMA-derived tumor volume (PSMA-TV) was defined as the total volume of whole-body PSMA-avid tumor lesions, and prostate PSMA-TV was defined as the volume of prostate PSMA-avid tumor lesions. Spearman's correlation was used to analyze the relationships between whole-body PSMA-TV and clinicopathological characteristics. The primary endpoint was progression-free survival (PFS), and Cox regression analyses were performed to explore the independent predictors for PFS.
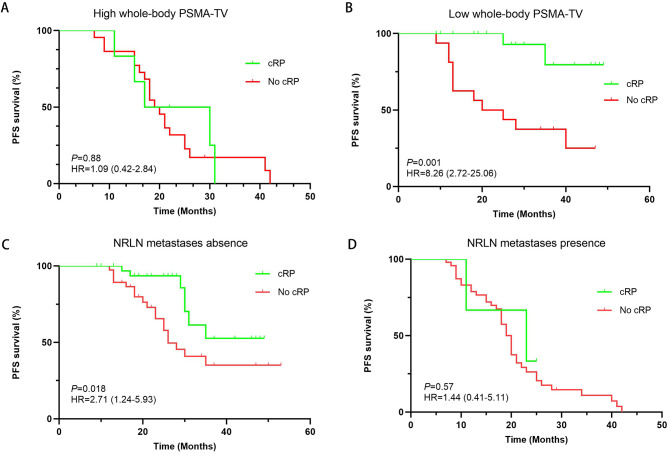
Results: Among 122 patients, 37 (30.32%) underwent systemic therapy plus cRP. The median and optimal cutoff values of the whole-body PSMA-TV were 71.68 cm3 (41.28-157.41 cm3) and 78.57 cm3, respectively. Whole-body PSMA-TV was positively correlated with prostate-specific antigen (PSA), and patients with nonregional lymph node (NRLN) metastases had a greater whole-body PSMA-TV (P = 0.001). Cox regression analyses revealed that cRP, lower whole-body PSMA-TV and the absence of NRLN metastases were associated with better PFS (all P < 0.05). Subgroup analyses revealed that patients with a low whole-body PSMA or no NRLN metastases had a significant improvement in PFS for cRP versus no cRP (HR: 8.26; 95% CI: 2.72-25.06, P = 0.001; HR: 2.71; 95% CI: 1.25-5.93, P = 0.018). Moreover, among patients with higher prostate PSMA-TV and prostate PSMA-TV/whole-body PSMA-TV, cRP also significantly prolonged PFS compared with those without cRP (HR: 3.49; 95% CI: 1.49-8.18, P = 0.004; HR: 8.54; 95% CI: 2.47-29.50, P = 0.013).
Conclusion: In management of primary low-volume mHSPC, whole-body and prostate PSMA-TV evaluations based on 18F-PSMA-1007 PET/CT could be helpful to identify the most suitable candidates for cRP.
Trial registration: Retrospectively registered.
Keywords: 18F-PSMA-1007 PET/CT; Cytoreductive radical prostatectomy; Low-volume mHSPC; Nonregional lymph node metastases; PSMA-TV.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures performed in the study and involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This retrospective analysis was approved by the Institutional Review Board of the First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, P.R. China. Informed consent was obtained from all individual participants included in the study. Consent for publication: Written informed consent was obtained from the patient for publication of this study and accompanying images. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
A visual whole-body tumor-burden classification based on PSMA PET/CT to predict response to novel androgen receptor signaling inhibitors for metastatic hormone-sensitive prostate cancer patients.Eur J Nucl Med Mol Imaging. 2025 Apr 25. doi: 10.1007/s00259-025-07300-4. Online ahead of print. Eur J Nucl Med Mol Imaging. 2025. PMID: 40278858
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Impact of non-regional lymph node metastases accurately revealed on 18F-PSMA-1007 PET/CT in the clinical management of metastatic hormone-sensitive prostate cancer.EJNMMI Res. 2023 Jul 6;13(1):64. doi: 10.1186/s13550-023-01009-x. EJNMMI Res. 2023. PMID: 37410264 Free PMC article.
-
68Ga-Labeled Prostate-specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-analysis.Eur Urol Focus. 2018 Sep;4(5):686-693. doi: 10.1016/j.euf.2016.11.002. Epub 2016 Nov 15. Eur Urol Focus. 2018. PMID: 28753806
-
Use of gallium-68 prostate-specific membrane antigen positron-emission tomography for detecting lymph node metastases in primary and recurrent prostate cancer and location of recurrence after radical prostatectomy: an overview of the current literature.BJU Int. 2020 Feb;125(2):206-214. doi: 10.1111/bju.14944. Epub 2019 Nov 29. BJU Int. 2020. PMID: 31680398 Free PMC article. Review.
Cited by
-
Advances in Current Treatment Paradigms for Metastatic Hormone-Sensitive Prostate Cancer.J Clin Med. 2025 Apr 8;14(8):2565. doi: 10.3390/jcm14082565. J Clin Med. 2025. PMID: 40283395 Free PMC article. Review.
References
-
- Culp MB, Soerjomataram I, Efstathiou JA, Bray F, Jemal A. Recent global patterns in prostate Cancer incidence and mortality rates. Eur Urol. 2020;77(1):38–52. - PubMed
-
- Prostate Cancer. [https://www.ncbi.nlm.nih.gov/books/NBK470550/].
-
- Yaxley JW, Raveenthiran S, Nouhaud FX, Samaratunga H, Yaxley WJ, Coughlin G, Yaxley AJ, Gianduzzo T, Kua B, McEwan L, et al. Risk of metastatic disease on (68) gallium-prostate-specific membrane antigen positron emission tomography/computed tomography scan for primary staging of 1253 men at the diagnosis of prostate cancer. BJU Int. 2019;124(3):401–7. - PubMed
-
- Matsumura N, Fujita K, Nishimoto M, Minami T, Tahara H, Yoshimura K, Uemura H. Current status and future perspectives of the managements of metastatic hormone-sensitive prostate cancer. World J Urol. 2023;41(8):2063–8. - PubMed
-
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate Cancer: long-term survival analysis of the Randomized Phase III E3805 CHAARTED trial. J Clin Oncol. 2018;36(11):1080–7. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
