

E Before A: Awake Bi-femoral Veno-Venous Extracorporeal Membrane Oxygenation as a Bridge to the Bifurcation Tracheal Y Stent
- PMID: 39902016
- PMCID: PMC11788711
- DOI: 10.7759/cureus.76890
E Before A: Awake Bi-femoral Veno-Venous Extracorporeal Membrane Oxygenation as a Bridge to the Bifurcation Tracheal Y Stent
Abstract
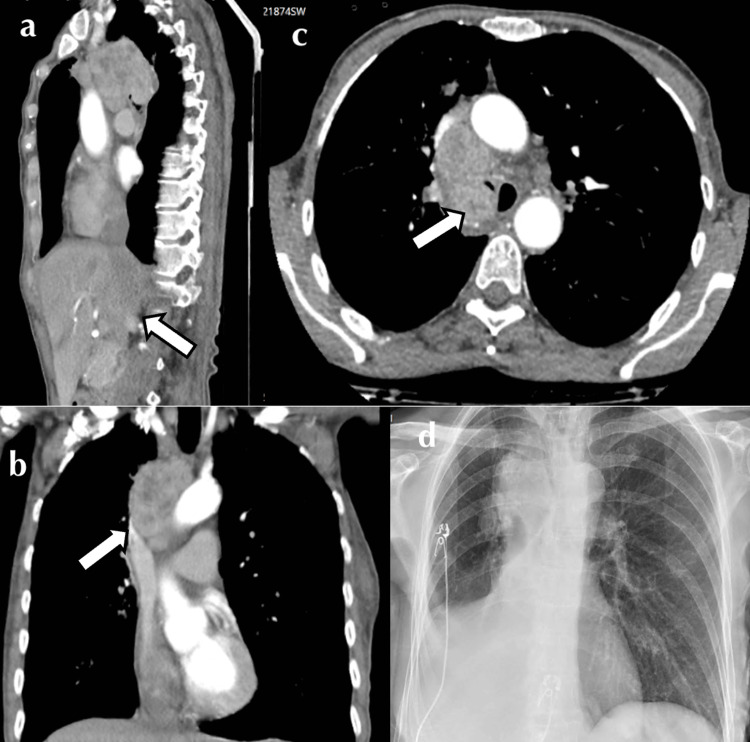
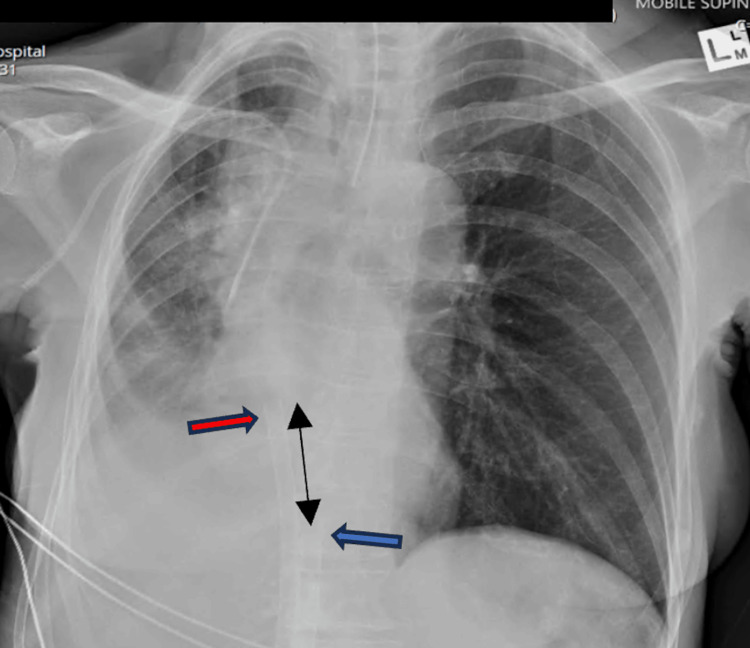
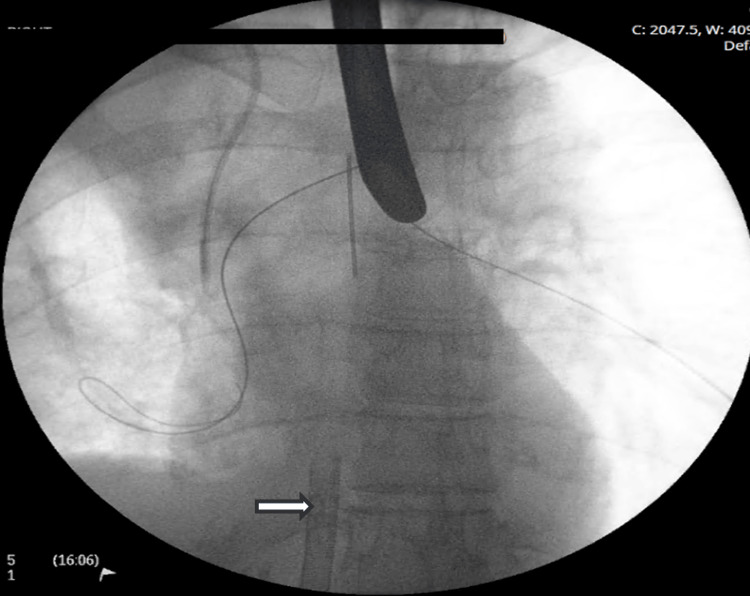
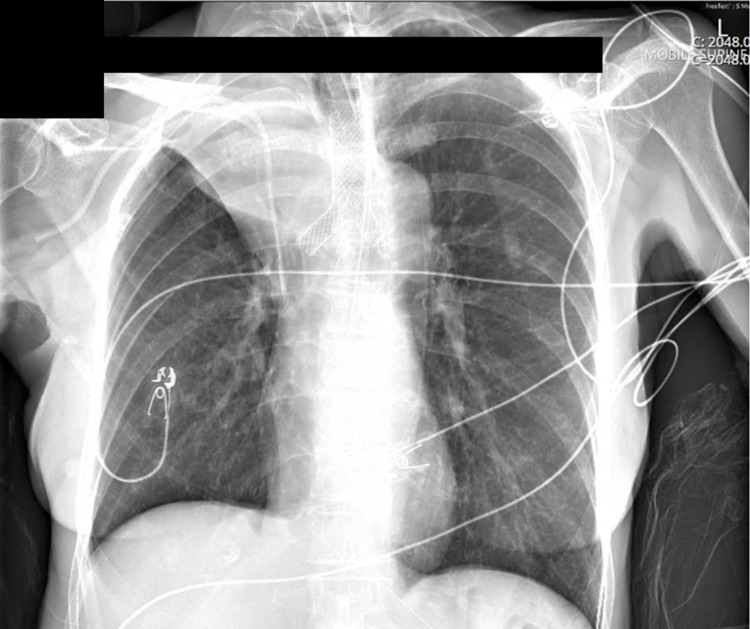
A 64-year-old female presented with severe respiratory failure secondary to a high-grade non-small lung cancer (IIIA NSCLC) causing extrinsic and intrinsic compression of the right main bronchus. She remained hypoxic despite 100% FiO2 delivery by high-flow nasal cannula and was considered at high risk of airway loss at intubation. Tumor debulking, histological diagnosis, and restoration of airway patency were facilitated with peri-procedural veno-venous extracorporeal membrane oxygen support (VVECMO). We describe a case of awake bifemoral VVECMO cannulation performed uneventfully as a bridge to the palliative placement of a self-expanding tracheal Y stent. The circuit was maintained in the absence of systemic anticoagulation. After less than 24 hours of extracorporeal support, the patient was decannulated, liberated from supplementary oxygen, and discharged from intensive care. The patient is now receiving platinum-based chemoradiotherapy and is eligible for targeted consolidative immunotherapy. As therapies and practice evolve, extracorporeal support may serve as a bridge to palliative interventions intended to salvage and improve the quality of life in oncology patients. Awake cannulation is feasible and may be preferred in cases of malignant airway obstruction.
Keywords: airway procedures; awake technique; central airway obstruction; hypoxic respiratory failure; non-small cell lung carcinoma (nsclc); tracheal stenting; veno-venous extracorporeal membrane oxygenation (vv ecmo).
Copyright © 2025, Worku et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Sydney Local Health District issued approval NA. This research conforms to the low-/negligible-risk pathway and is exempt from ethical consideration. . Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Elective use of veno-venous extracorporeal membrane oxygenation and high-flow nasal oxygen for resection of subtotal malignant distal airway obstruction.Anaesth Intensive Care. 2017 Jan;45(1):88-91. doi: 10.1177/0310057X1704500113. Anaesth Intensive Care. 2017. PMID: 28072940
-
Extracorporeal lung support technologies - bridge to recovery and bridge to lung transplantation in adult patients: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(5):1-47. Epub 2010 Apr 1. Ont Health Technol Assess Ser. 2010. PMID: 23074408 Free PMC article.
-
Tracheostomy and venovenous extracorporeal membrane oxygenation for difficult airway patient with carinal melanoma: A case report and literature review.World J Clin Cases. 2022 Dec 16;10(35):13088-13098. doi: 10.12998/wjcc.v10.i35.13088. World J Clin Cases. 2022. PMID: 36569026 Free PMC article.
-
Local Anesthetic Infiltration, Awake Veno-Venous Extracorporeal Membrane Oxygenation, and Airway Management for Resection of a Giant Mediastinal Cyst: A Narrative Review and Case Report.J Clin Med. 2024 Dec 30;14(1):165. doi: 10.3390/jcm14010165. J Clin Med. 2024. PMID: 39797248 Free PMC article. Review.
-
Veno-venous extracorporeal membrane oxygenation: cannulation techniques.J Thorac Dis. 2016 Dec;8(12):3762-3773. doi: 10.21037/jtd.2016.12.88. J Thorac Dis. 2016. PMID: 28149575 Free PMC article. Review.
References
-
- Use of combined suspension laryngoscopy and jet ventilation for Y-shaped airway stents delivery. Monnier Y, Chollet-Rivier M, Gonzalez M, Nicod L, Simon C, Lovis A. Ann Thorac Surg. 2014;97:2208–2210. - PubMed
-
- A multicenter experience with the placement of self-expanding metallic tracheobronchial Y stents. Madan K, Dhooria S, Sehgal IS, et al. J Bronchology Interv Pulmonol. 2016;23:29–38. - PubMed
-
- Venoarterial-extracorporeal membrane oxygenation without routine systemic anticoagulation decreases adverse events. Wood KL, Ayers B, Gosev I, Kumar N, Melvin AL, Barrus B, Prasad S. Ann Thorac Surg. 2020;109:1458–1466. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials