

New Insights into Ruling Out Internal Herniations After Laparoscopic Gastric Bypass on the Abdominal CT Scan: The OPERATE study
- PMID: 39903413
- PMCID: PMC11906499
- DOI: 10.1007/s11695-025-07715-w
New Insights into Ruling Out Internal Herniations After Laparoscopic Gastric Bypass on the Abdominal CT Scan: The OPERATE study
Abstract
Background: Internal herniation (IH) is a potentially life-threatening complication after gastric bypass. Accurate diagnosis of IH remains challenging. This study aims to validate the Eindhoven2020 (EHV20) scoring system for ruling out IH and seeks to improve its diagnostic accuracy through additional radiologic parameters.
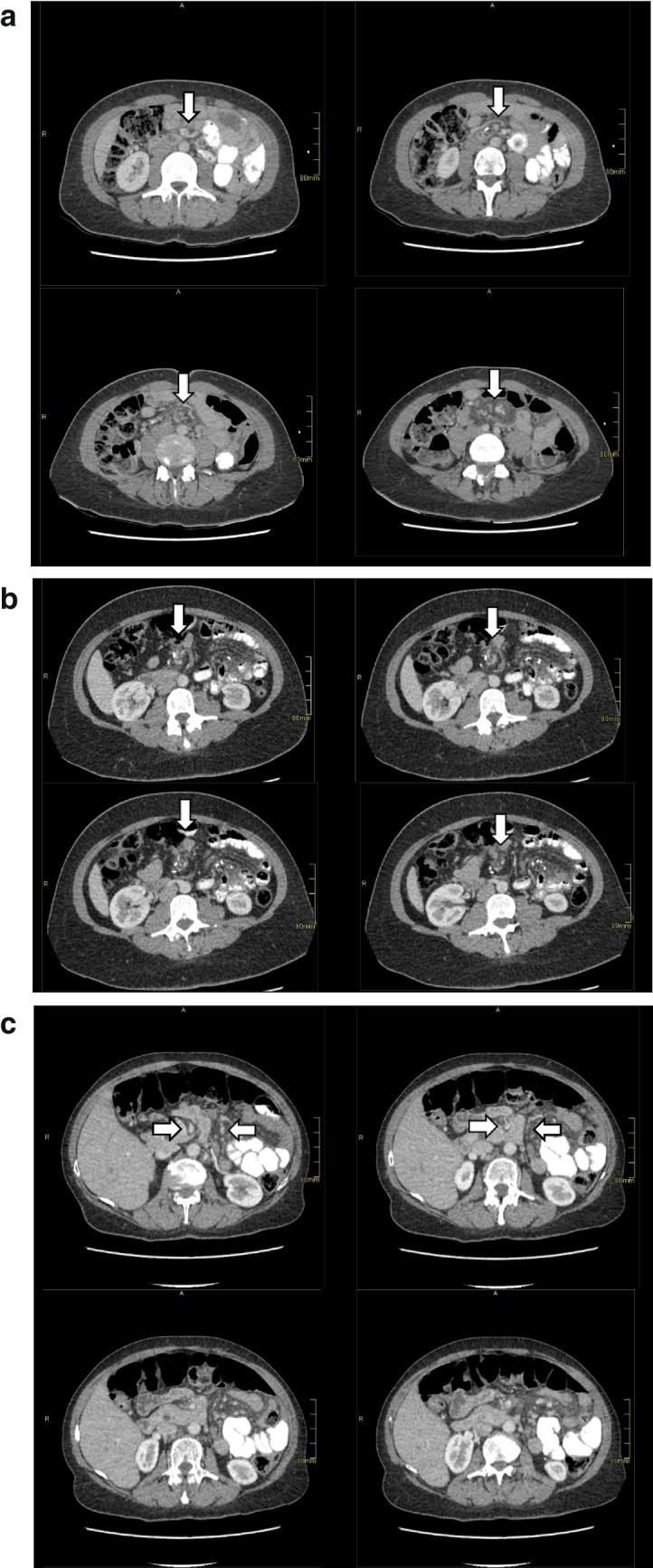
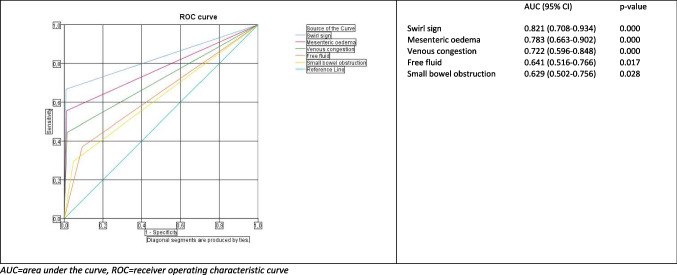
Methods: Patients participating in a prospective study on abdominal pain after gastric bypass surgery were selected if a CT scan was performed. CT scans were scored following the EHV20 scoring system containing ten signs of IH to confirm the individual and collective accuracy of these signs. Also, we evaluated the diagnostic value of additional radiologic parameters: delayed passage of contrast, dilated intestinal loops, and free fluid.
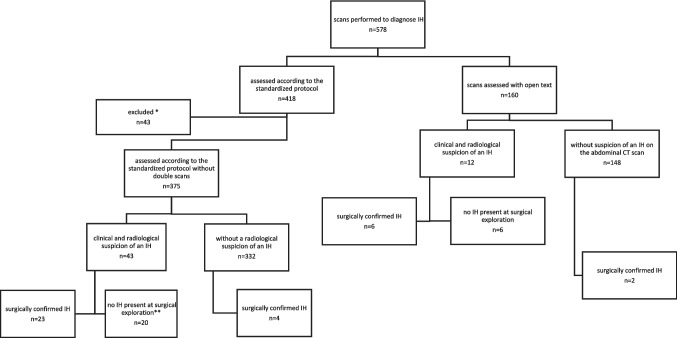
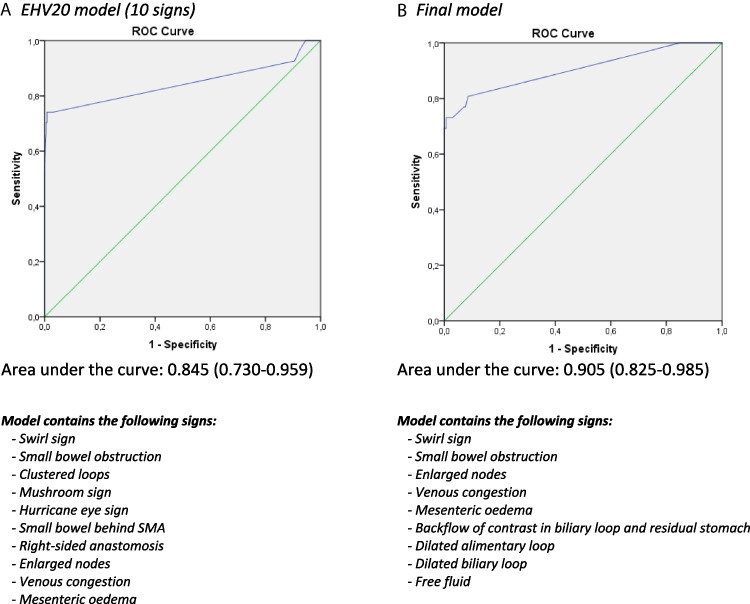
Results: A total of 375 patients with abdominal pain were included. IH was confirmed during laparoscopy in 27 patients. On CT, the highest sensitivity was achieved by the swirl sign (66.7%) and the highest specificity by a small bowel behind the superior mesenteric artery (99.7%). The area under the receiver operating characteristic curve (AUC) based on the EHV20 scoring system for ruling out IH was 0.845 (95% CI 0.730-0.959). The AUC could be improved to 0.905 (95% CI 0.825-0.985) (p = 0.088) through the incorporation of several additional signs. Overall, this new scoring system included swirl sign, small bowel obstruction, enlarged nodes, venous congestion, mesenteric edema, dilated alimentary or biliary loop, free fluid, and backward flow in the biliary loop with possible backflow in the residual stomach.
Conclusions: Incorporation of additional CT signs into an existing scoring system can help clinicians to safely rule out IH in patients with abdominal pain after bariatric surgery.
Keywords: Computed tomography; Internal herniation; Radiological signs; Standardized protocol.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: The authors declare no competing interests.
Figures
Similar articles
-
Role of CT imaging in discriminating internal hernia from aspecific abdominal pain following Roux-en-Y gastric bypass: a single high-volume centre experience.Updates Surg. 2020 Dec;72(4):1115-1124. doi: 10.1007/s13304-020-00767-w. Epub 2020 Apr 18. Updates Surg. 2020. PMID: 32306275
-
Structured CT reporting improves accuracy in diagnosing internal herniation after laparoscopic Roux-en-Y gastric bypass.Eur Radiol. 2020 Jun;30(6):3448-3454. doi: 10.1007/s00330-020-06688-x. Epub 2020 Feb 20. Eur Radiol. 2020. PMID: 32078011 Free PMC article.
-
Internal Hernia after Laparoscopic Roux-en-Y Gastric Bypass: Optimal CT Signs for Diagnosis and Clinical Decision Making.Radiology. 2017 Mar;282(3):752-760. doi: 10.1148/radiol.2016160956. Epub 2016 Sep 30. Radiology. 2017. PMID: 27689925
-
The Diagnostic Accuracy of Abdominal Computed Tomography in Diagnosing Internal Herniation Following Roux-en-Y Gastric Bypass Surgery: A Systematic Review and Meta-analysis.Ann Surg. 2022 May 1;275(5):856-863. doi: 10.1097/SLA.0000000000005247. Epub 2021 Oct 8. Ann Surg. 2022. PMID: 35129527
-
Internal herniation after Roux-en-Y gastric bypass: case reports and a review of the literature.Acta Chir Belg. 2009 May-Jun;109(3):385-91. doi: 10.1080/00015458.2009.11680444. Acta Chir Belg. 2009. PMID: 19943598 Review.
References
-
- Iannuccilli JD, Grand D, Murphy BL, et al. Sensitivity and specificity of eight CT signs in the preoperative diagnosis of internal mesenteric hernia following Roux-en-Y gastric bypass surgery. Clin Radiol. 2009;64(4):373–80. - PubMed
-
- Lockhart ME, Tessler FN, Canon CL, et al. Internal hernia after gastric bypass: sensitivity and specificity of seven CT signs with surgical correlation and controls. AJR Am J Roentgenol. 2007;188(3):745–50. - PubMed
-
- Gormsen J, Burcharth J, Gogenur I, et al. Prevalence and risk factors for chronic abdominal pain after Roux-en-Y gastric bypass surgery: a cohort study. Ann Surg. 2021;273(2):306–14. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
