

Exercise-based cardiac rehabilitation for patients undergoing coronary artery operation: a systematic review and meta-analysis based on current randomized controlled trials
- PMID: 39903572
- PMCID: PMC12372725
- DOI: 10.1097/JS9.0000000000002268
Exercise-based cardiac rehabilitation for patients undergoing coronary artery operation: a systematic review and meta-analysis based on current randomized controlled trials
Abstract
Background: Currently, exercise-based cardiac rehabilitation (CR) has been receiving increasing interest for its potentially beneficial effects on the health related quality of life (HRQoL) and outcomes of patients with coronary heart disease (CHD). The aim of this study was to evaluate the effect of exercise-based CR on patients after coronary artery bypass graft (CABG) and percutaneous coronary interventions (PCI).
Methods: We searched PubMed, Embase, Cochrane Library, and Web of Science from inception to 1 December 2023 for relevant studies that evaluated the effect of exercise-based CR on patients after CABG and PCI. Our primary outcomes included mortality, complications, hospital admissions, and HRQoL between patients receiving exercise-based CR and usual care. All statistical analyses were performed using the standard statistical procedures provided in Review Manager 5.2 and Stata 12.0.
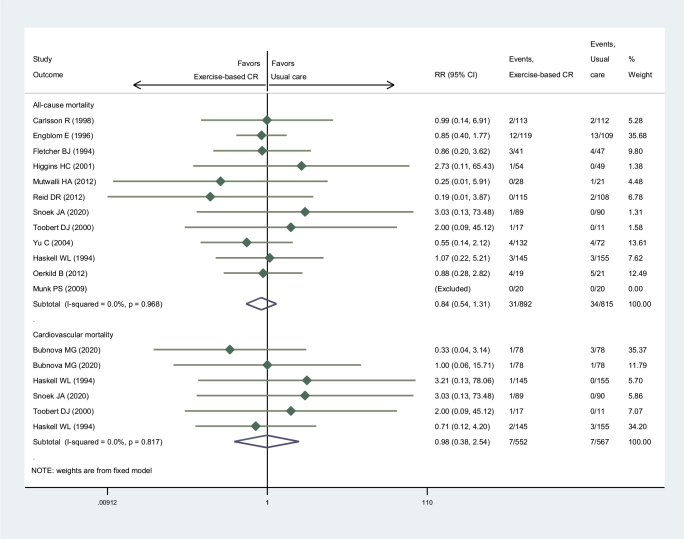
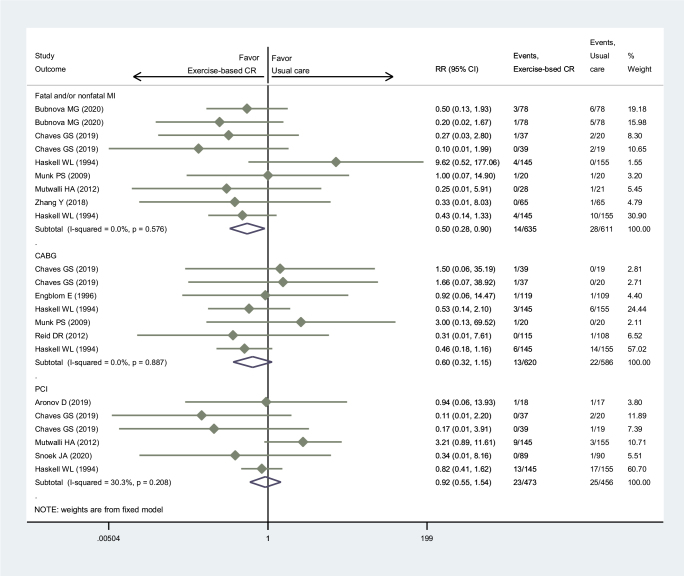
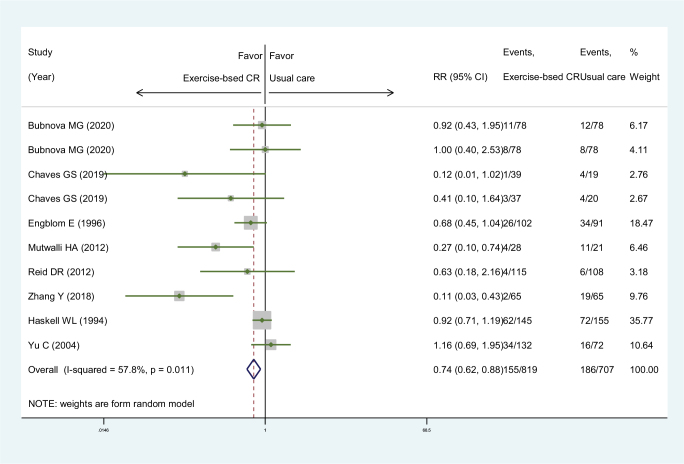
Results: We finally indicated and included 25 randomized controlled trials (RCTs) with 4106 participants for the present analysis. Our pooled results indicated that, compared to usual care, exercise-based CR did not increase the all-cause (relative risk, RR: 0.84; 95% confidence interval, CI: 0.54-1.31) and cardiovascular (RR: 0.98; 95% CI: 0.38-2.54) mortality for patients after coronary artery operation. Similarly, exercise-based CR had an equal effect on coronary artery complications for patients after coronary artery surgery, including CABG (RR: 0.60; 95% CI: 0.32 ‒ 1.15) and PCI (RR: 0.92; 95% CI: 0.55-1.54). It was indicated that exercise-based CR significantly reduced the incidence of myocardial infarction (MI) by half with an RR of 0.50 (95% CI: 0.28-0.90). In addition, exercise-based CR also significantly reduced all-cause hospital admissions with an RR of 0.74 (95% CI: 0.62-0.88). Compared to usual care, exercise-based CR obviously improved HRQoL of patients after coronary artery operation evaluated with SF-36 summary scores (standardized mean difference, SMD: 0.24; 95% CI: 0.11-0.38) and SF-36 8 domains (SMD: 0.35; 95% CI: 0.24-0.46).
Conclusions: Our analysis indicated that exercise-based CR had a significant effect on the improvement of HRQoL in patients after coronary artery surgeries without increasing mortality or the incidence of re-intervention with operations.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no relevant conflict of interest.
Figures




References
-
- Meirhaeghe A, Montaye M, Biasch K, et al. Coronary heart disease incidence still decreased between 2006 and 2014 in France, except in young age groups: results from the French MONICA registries. Eur J Prev Cardiol 2020;27:1178–86. - PubMed
-
- World Health Organization. Global health estimates 2016: deaths by cause, age, sex, by country and by region, 2000-2016. www.who.int/healthinfo/global_burden_disease/estimates/en/ (accessed prior to 12 October 2021).
-
- Hannan EL, Wu Y, Harik L, et al. Coronary artery bypass surgery vs. percutaneous interventions for women with multivessel coronary artery disease. J Thorac Cardiovasc Surg 2024;168:863–872.e8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
