

Trends, gender, and racial disparities in patients with mortality due to paroxysmal tachycardia: A nationwide analysis from 1999-2020
- PMID: 39903690
- PMCID: PMC11793763
- DOI: 10.1371/journal.pone.0314715
Trends, gender, and racial disparities in patients with mortality due to paroxysmal tachycardia: A nationwide analysis from 1999-2020
Abstract
Background: Paroxysmal tachycardia encompasses various heart rhythm disorders that cause rapid heart rates. Its episodic occurrence makes it difficult to identify and measure its prevalence and trends in the population. Additionally, there is limited data on disparities and trends in mortality due to paroxysmal tachycardia, which is essential for assessing current medical approaches and identifying at-risk populations.
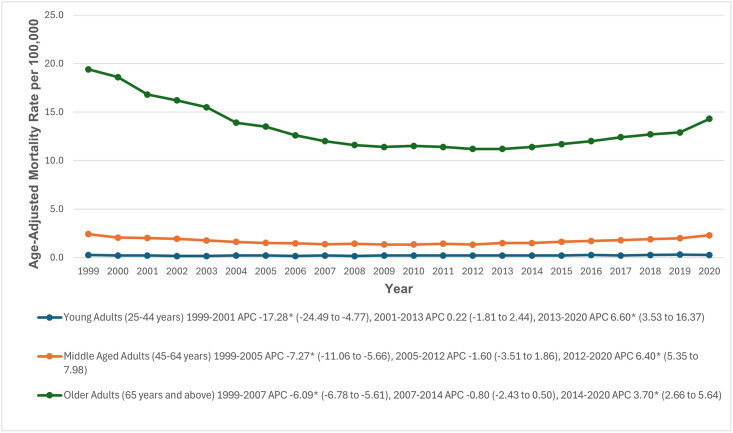
Methods: Our study examined death certificates from 1999 to 2020 using the CDC WONDER Database to identify deaths caused by paroxysmal tachycardia in individuals aged 25 and older, using the ICD-10 code I47. Age-adjusted mortality rates (AAMRs) and annual percent changes (APC) were calculated by year, gender, age group, race/ethnicity, geographic location, and urbanization status. Trends in AAMRs were analyzed using the Joinpoint Regression Program to identify significant changes and inflection points in mortality trends throughout the study period.
Results: Between 1999 and 2020, 155,320 deaths were reported in patients with paroxysmal tachycardia. Overall, AAMR decreased from 4.8 to 3.7 per 100,000 population between 1999 and 2020, despite showing a significant increase from 2014 to 2020 (APC: 4.33; 95% CI: 3.53 to 5.56). Men had consistently higher AAMRs than women (4.7 vs. 2.2). Furthermore, we found that AAMRs were highest among Non-Hispanic (NH) Black or African Americans and lowest in NH Asian or Pacific Islanders (4 vs. 1.9). Nonmetropolitan areas had higher AAMRs than metropolitan areas (3.6 vs. 3.2).
Conclusions: Our analysis showed a significant decrease in mortality from paroxysmal tachycardia since 1999, although there has been a slight increase in recent years. However, disparities remain, with higher AAMRs among men, NH Black or African Americans, and residents of non-metropolitan areas. These findings call for immediate public health actions to curb the rising trends and reduce potential disparities.
Copyright: © 2025 Goyal et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Kaplan J, Kanwal A, Ahmed I, Lala V. Reentrant Arrhythmias. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. [cited 2024 Oct 22]. http://www.ncbi.nlm.nih.gov/books/NBK557775/
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
