

Weight development in children with obesity without treatment: A Danish cohort study with long-term follow-up
- PMID: 39904846
- PMCID: PMC12001306
- DOI: 10.1111/ijpo.70001
Weight development in children with obesity without treatment: A Danish cohort study with long-term follow-up
Abstract
Introduction: Limited insight exists into the weight development in children with obesity not receiving obesity treatment.
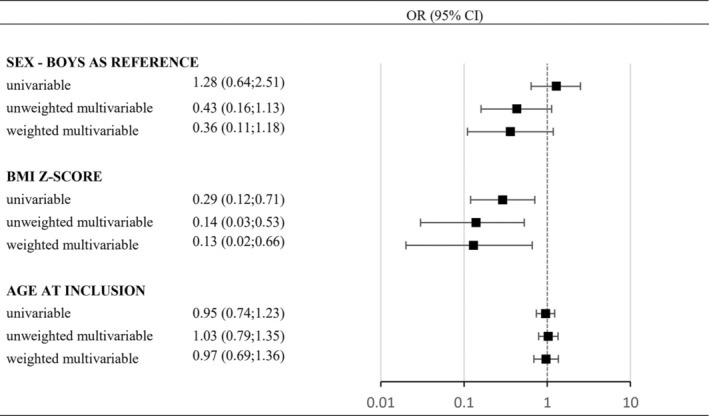
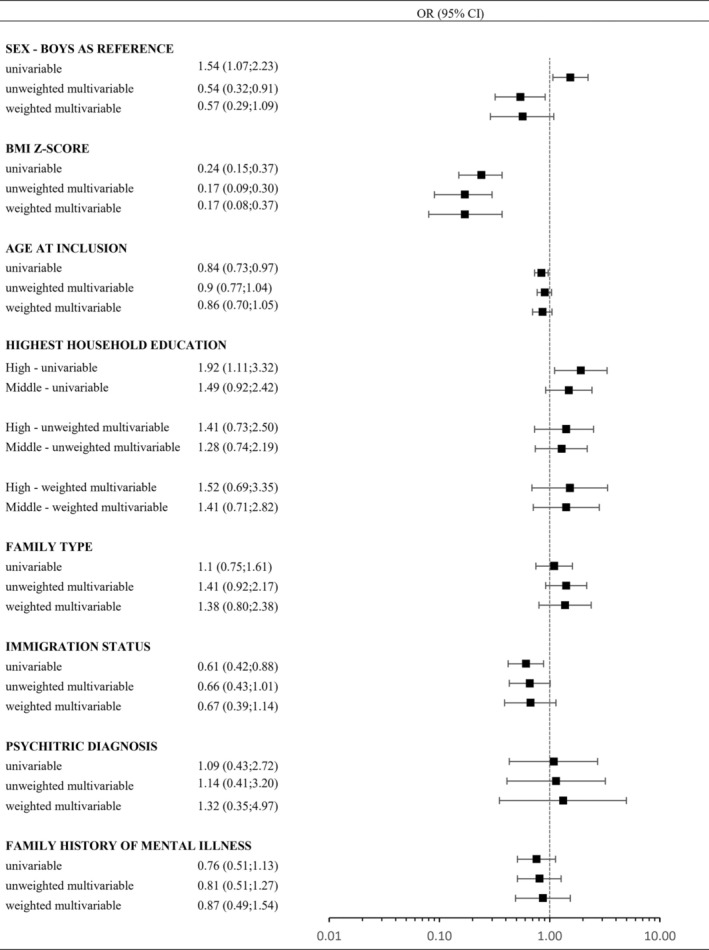
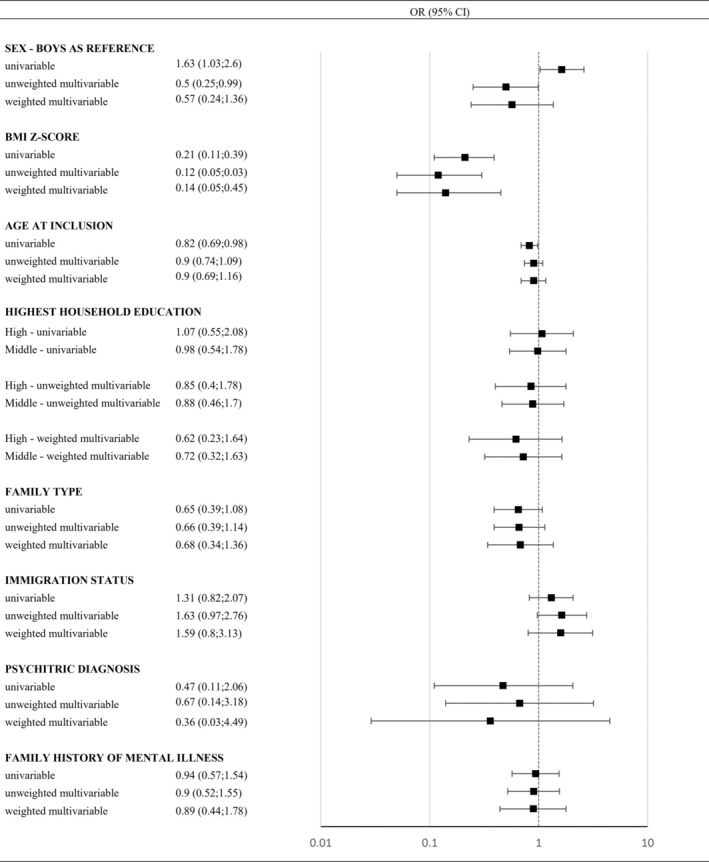
Methods: This cohort study included 467 Danish children aged 5-10 years with obesity (iso-BMI >30 kg/m2) not receiving treatment. Data from mandatory health check-ups on school-children's height and weight (converted to BMI z-scores) were merged with the Danish National Registries. A multivariable logistic regression weighted for the duration of follow-up was used to estimate odds ratios (OR) for normalization of BMI (iso-BMI 18.5-25 kg/m2) and obesity remission (iso-BMI 18.5-30 kg/m2).
Results: During a median follow-up of more than 6 years, 7.9% of the children normalized their BMI, while 45.4% obtained obesity remission. BMI z-score at inclusion acted as a strong inverse predictor for normalizing BMI (OR 0.14 per one-unit SD, CI: 0.03-0.53) and for obesity remission (OR 0.17 per one-unit SD, CI: 0.08-0.37). No other significant predictors were observed in the weighted multivariable models.
Conclusion: Higher BMI z-scores inversely predict normalizing BMI and achieving obesity remission in untreated children. Given that many children naturally achieve obesity remission or weight normalization, resources should focus on understanding barriers of obesity maintenance and to develop effective strategies for those who do not experience improvement.
© 2025 The Author(s). Pediatric Obesity published by John Wiley & Sons Ltd on behalf of World Obesity Federation.
Conflict of interest statement
All authors (except for IIA and LM) are employed at Steno Diabetes Center Aarhus, Aarhus University Hospital, a public hospital and research institution situated in the Central Denmark Region, which is partly funded by an unrestricted grant from the Novo Nordisk Foundation.
Figures

Similar articles
-
Long-Term Change in BMI for Children with Obesity Treated in Family-Centered Lifestyle Interventions.Obes Facts. 2024;17(6):570-581. doi: 10.1159/000540389. Epub 2024 Sep 12. Obes Facts. 2024. PMID: 39265552 Free PMC article.
-
Association of Birth Weight, Childhood Body Mass Index, and Height With Risk of Hidradenitis Suppurativa.JAMA Dermatol. 2020 Jul 1;156(7):746-753. doi: 10.1001/jamadermatol.2020.1047. JAMA Dermatol. 2020. PMID: 32347905 Free PMC article.
-
Effects of a multidisciplinary weight loss intervention in overweight and obese children and adolescents: 11 years of experience.PLoS One. 2017 Jul 13;12(7):e0181095. doi: 10.1371/journal.pone.0181095. eCollection 2017. PLoS One. 2017. PMID: 28704494 Free PMC article.
-
The effectiveness of web-based programs on the reduction of childhood obesity in school-aged children: A systematic review.JBI Libr Syst Rev. 2012;10(42 Suppl):1-14. doi: 10.11124/jbisrir-2012-248. JBI Libr Syst Rev. 2012. PMID: 27820152
-
[Simple obesity in children. A study on the role of nutritional factors].Med Wieku Rozwoj. 2006 Jan-Mar;10(1):3-191. Med Wieku Rozwoj. 2006. PMID: 16733288 Review. Polish.
References
-
- Buttitta M, Iliescu C, Rousseau A, Guerrien A. Quality of life in overweight and obese children and adolescents: a literature review. Qual Life Res. 2014;23(4):1117‐1139. - PubMed
-
- Schwimmer JB, Burwinkle TM, Varni JW. Health‐related quality of life of severely obese children and adolescents. Jama. 2003;289(14):1813‐1819. - PubMed
-
- Bjerregaard LG, Adelborg K, Baker JL. Change in body mass index from childhood onwards and risk of adult cardiovascular disease. Trends Cardiovasc Med. 2019;30(1):39‐45. - PubMed
-
- Bjerregaard LG, Jensen BW, Angquist L, Osler M, Sorensen TIA, Baker JL. Change in overweight from childhood to early adulthood and risk of type 2 diabetes. N Engl J Med. 2018;378(14):1302‐1312. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
