

Right ventricular dysfunction for prediction of long-term recovery in de novo HFrEF : a PROLONG-II substudy
- PMID: 39905162
- PMCID: PMC12055338
- DOI: 10.1002/ehf2.15236
Right ventricular dysfunction for prediction of long-term recovery in de novo HFrEF : a PROLONG-II substudy
Abstract
Aims: To analyse the predictive value of advanced markers of right ventricular (RV) function and RV-pulmonary arterial (PA) coupling in forecasting long-term left ventricular (LV) improvement in de novo heart failure with reduced ejection fraction (HFrEF).
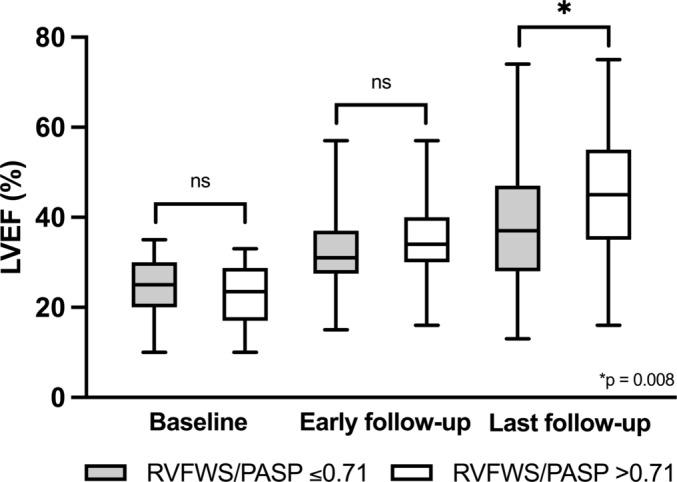
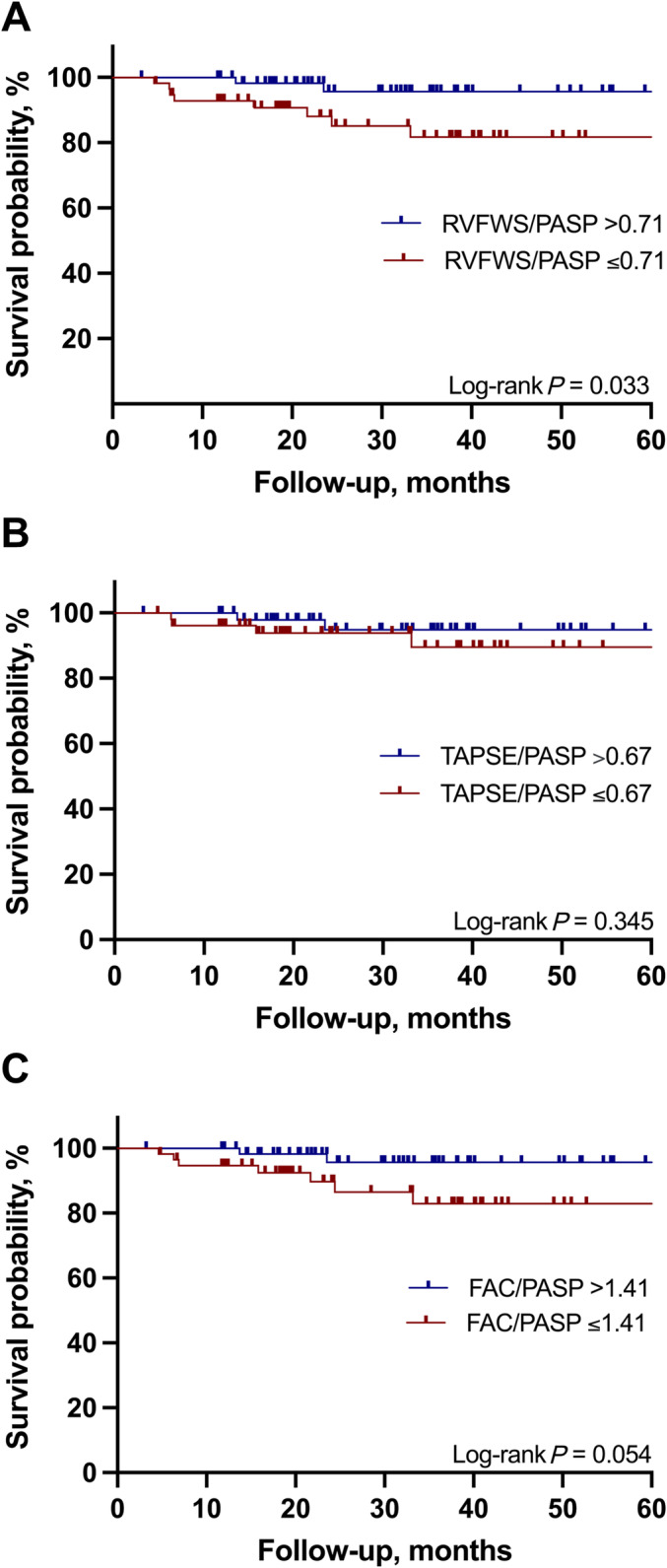
Methods and results: 260 patients (mean age 57 years, 68% men) from the PROLONG-II study were included. PROLONG-II analysed patients with new-onset HFrEF receiving a wearable cardioverter-defibrillator. For this substudy, RV free wall longitudinal strain (RVFWS), tricuspid annular plane systolic excursion (TAPSE), fractional area change (FAC), and right ventricular-pulmonary artery (RV-PA) coupling ratios [RVFWS/systolic pulmonary artery pressure (PASP), TAPSE/PASP and FAC/PASP] at baseline and 3-month follow-up (early follow-up) were examined. LV improvement and non-improvement were defined as an LV ejection fraction (LVEF) of >35% or ≤35% at last available (long-term) follow-up. The median follow-up was 31.5 months (IQR: 18.2-45.4), and 151 (58%) patients experienced LV improvement in the long term. No significant differences of RV function and markers of RV-PA coupling were observed at baseline; however, the subgroup of patients with long-term LVEF improvement showed better RV function at early follow-up (RVFWS -20.9 ± 4.3 vs. -18.5 ± 5.1%, TAPSE 19.7 ± 5.1 vs. 17.4 ± 4.9 mm, FAC 39.7 ± 8.5 vs. 35.2 ± 9.4%, all P < 0.01). In multivariable analysis, RVFWS at early follow-up was shown to be an independent predictor of later LV recovery [odds ratio 1.078 (95% confidence interval 1.010-1.150), P < 0.05]. The non-improvers exhibited worse RV-PA coupling at early follow-up [RVFWS/PASP 0.82 ± 0.35 vs. 0.65 ± 0.35%/mmHg, TAPSE/PASP 0.71 (0.55-1.00) vs. 0.54 (0.35-0.75) mm/mmHg, FAC/PASP 1.54 ± 0.61 vs. 1.24 ± 0.75%/mmHg, all P < 0.01]. RVFWS/PASP identified RV-PA uncoupling was associated with a higher risk of all-cause mortality (hazard ratio 4.64, 95% confidence interval 1.34-16.09, P = 0.033).
Conclusions: Persistent RV dysfunction, as indicated by both standard and advanced echocardiographic markers during the early follow-up period, implies a reduced potential for long-term LV recovery in patients with newly diagnosed HFrEF.
Keywords: Heart failure; Right ventricular free wall longitudinal strain; Right ventricular function; Right ventricular‐pulmonary arterial coupling; Speckle‐tracking echocardiography.
© 2025 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
H.A.K.H. received modest lecture honorary and/or a fellowship grant from AstraZeneca, Zoll, and Boston Scientific. J.M. received modest lecture honorary, travel grants, and/or a fellowship grant from Abbott, Biotronik, Boston Scientific, and Zoll. J.E. received a fellowship grant from Biotronik. C.V. received honorary for lectures or consulting from Abbott, Medtronic, and Zoll. J.B. received honoraria for lectures/consulting from Novartis, Vifor, Bayer, Pfizer, Boehringer Ingelheim, AstraZeneca, Cardior, CVRx, BMS, Amgen, Corvia, Norgine, Edwards, and Roche not related to this article; and research support for the department from Zoll, CVRx, Abiomed, Norgine, and Roche, not related to this article. D.D. received modest lecture honorary, travel grants, and/or a fellowship grant from Abbott, AstraZeneca, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, CVRx, Medtronic, Microport, Pfizer, Sanofi, and Zoll. D.B. received honoraria for lectures/consulting from Abbott Vascular, AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Daiichi Sankyo, Edwards Lifesciences, and Pfizer. All other authors: none declared.
Figures
Similar articles
-
Right ventricular dysfunction in left-sided heart failure with preserved versus reduced ejection fraction.Eur J Heart Fail. 2017 Dec;19(12):1664-1671. doi: 10.1002/ejhf.873. Epub 2017 Jun 8. Eur J Heart Fail. 2017. PMID: 28597497
-
Right Ventricular-Pulmonary Artery Uncoupling and Strain in Acute Heart Failure.J Am Heart Assoc. 2025 May 6;14(9):e039858. doi: 10.1161/JAHA.124.039858. Epub 2025 May 2. J Am Heart Assoc. 2025. PMID: 40314350 Free PMC article.
-
Right ventricular function and its coupling to pulmonary circulation predicts exercise tolerance in systolic heart failure.ESC Heart Fail. 2022 Feb;9(1):450-464. doi: 10.1002/ehf2.13726. Epub 2021 Dec 24. ESC Heart Fail. 2022. PMID: 34953062 Free PMC article.
-
The prognostic impact of right ventricular-pulmonary arterial coupling in heart failure: a systematic review and meta-analysis.Heart Fail Rev. 2024 Jan;29(1):13-26. doi: 10.1007/s10741-023-10341-2. Epub 2023 Aug 28. Heart Fail Rev. 2024. PMID: 37639067 Free PMC article.
-
Application of an echocardiographic index to characterize right ventricular-pulmonary arterial coupling in heart failure.ESC Heart Fail. 2024 Jun;11(3):1290-1304. doi: 10.1002/ehf2.14663. Epub 2024 Jan 16. ESC Heart Fail. 2024. PMID: 38229524 Free PMC article. Review.
References
-
- Carluccio E, Biagioli P, Alunni G, Murrone A, Zuchi C, Coiro S, et al. Prognostic value of right ventricular dysfunction in heart failure with reduced ejection fraction: superiority of longitudinal strain over tricuspid annular plane systolic excursion. Circ Cardiovasc Imaging 2018;11:e006894. doi:10.1161/CIRCIMAGING.117.006894 - DOI - PubMed
-
- Dini FL, Carluccio E, Simioniuc A, Biagioli P, Reboldi G, Galeotti GG, et al. Right ventricular recovery during follow‐up is associated with improved survival in patients with chronic heart failure with reduced ejection fraction. Eur J Heart Fail 2016;18:1462‐1471. doi:10.1002/ejhf.639 - DOI - PubMed
-
- Houard L, Benaets MB, de Meester de Ravenstein C, Rousseau MF, Ahn SA, Amzulescu MS, et al. Additional prognostic value of 2D right ventricular speckle‐tracking strain for prediction of survival in heart failure and reduced ejection fraction: a comparative study with cardiac magnetic resonance. JACC Cardiovasc Imaging 2019;12:2373‐2385. doi:10.1016/j.jcmg.2018.11.028 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
