

Upadacitinib in active non-radiographic axial spondyloarthritis: 2-year data from the phase 3 SELECT-AXIS 2 study
- PMID: 39905436
- PMCID: PMC11792409
- DOI: 10.1186/s13075-024-03441-3
Upadacitinib in active non-radiographic axial spondyloarthritis: 2-year data from the phase 3 SELECT-AXIS 2 study
Abstract
Background: In SELECT-AXIS 2, upadacitinib improved the signs and symptoms of active non-radiographic axial spondyloarthritis (nr-axSpA) through 52 weeks versus placebo and was well tolerated. Here, we evaluated the efficacy and safety of upadacitinib through 2 years.
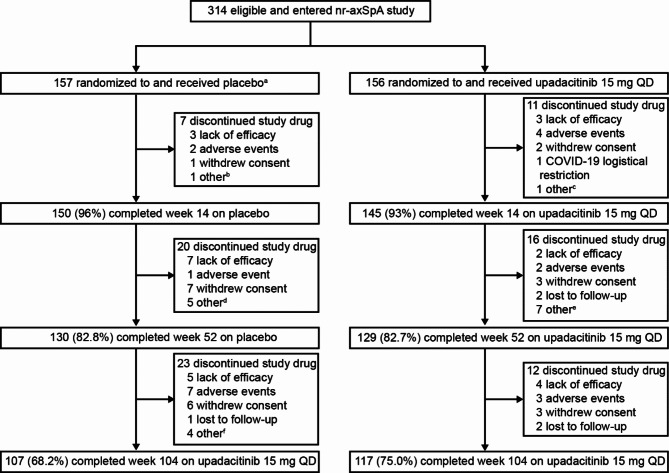
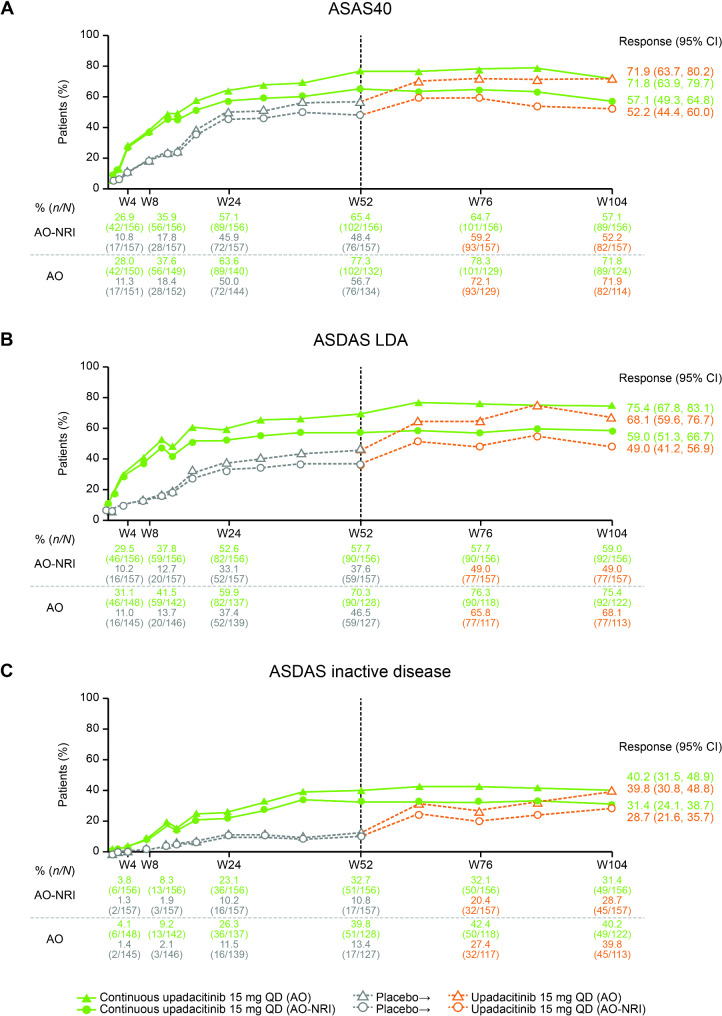
Methods: The study enrolled eligible adult patients with a clinical diagnosis of nr-axSpA who met the 2009 Assessment of SpondyloArthritis international Society (ASAS) classification criteria and had objective signs of active inflammation on magnetic resonance imaging (MRI) of sacroiliac joints and/or high-sensitivity C-reactive protein. Patients were randomized 1:1 to receive double-blinded treatment with upadacitinib 15 mg once daily (QD) or placebo for 52 weeks, after which all patients received open-label treatment with upadacitinib 15 mg QD. Efficacy results over 104 weeks were reported as observed (AO) and either AO with non-responder imputation (AO-NRI; binary endpoints) or AO with mixed-effect model for repeated measures (continuous endpoints). Treatment-emergent adverse events (TEAEs) were summarized through week 104.
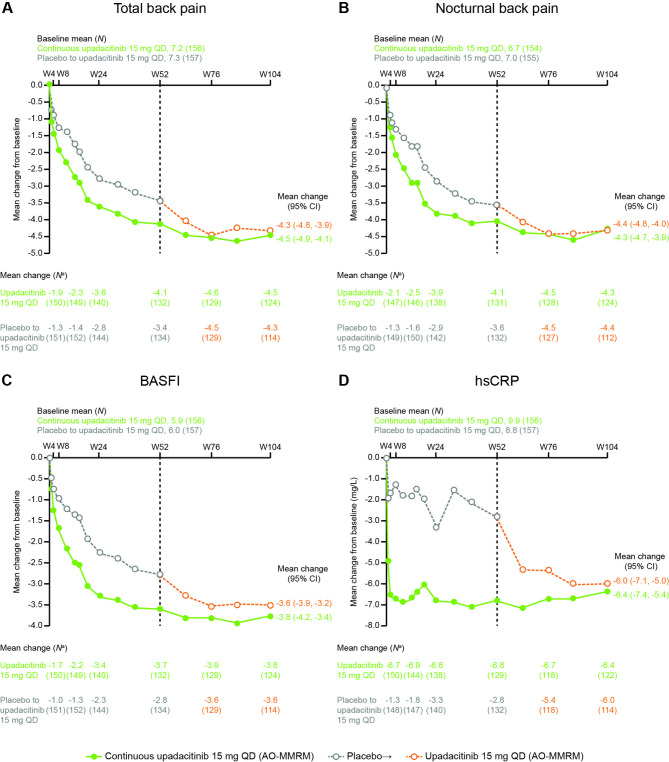
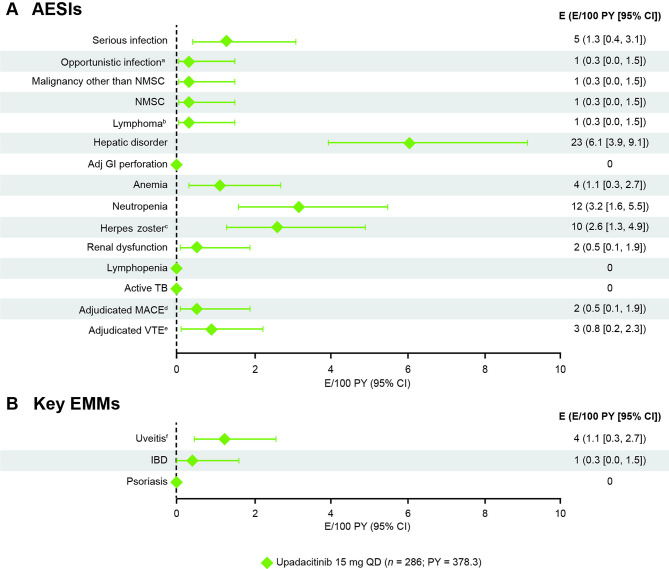
Results: Of 313 patients randomized and treated, 224 (continuous upadacitinib n = 117; placebo/upadacitinib n = 107) completed 104 weeks of treatment. In patients who received continuous upadacitinib, sustained improvement was observed through 2 years of treatment across efficacy endpoints including disease activity, pain, function, enthesitis, quality of life, and MRI measures of inflammation. At week 104, 57.1%, 59.0%, and 31.4% of patients achieved ASAS40 response, and low disease activity and inactive disease (as defined by Axial Spondyloarthritis Disease Activity Score), respectively (AO-NRI); week 104 outcomes were generally similar in patients who initially received placebo and were switched to upadacitinib at week 52. In total, 286 patients were exposed to ≥ 1 dose of upadacitinib, comprising 378.3 patient-years (PY) of exposure. Upadacitinib was generally well tolerated, with exposure-adjusted event rates (EAERs) for TEAEs, serious adverse events (AEs), and AEs leading to study drug discontinuation of 207.5, 8.7, and 5.3 events/100 PY, respectively. EAERs of TEAEs of special interest were broadly consistent with those reported through week 52.
Conclusions: Treatment with upadacitinib demonstrated consistent improvement and maintenance of treatment effect across efficacy endpoints through 2 years; no new safety signals were identified with additional exposure.
Trial registration: NCT04169373.
Keywords: Axial spondyloarthritis; Disease activity; Inflammation; Janus kinase inhibitor; Safety; Upadacitinib.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted according to the International Council for Harmonisation guidelines and the Declaration of Helsinki. The trial protocol was approved by independent ethics committees and institutional review boards. Written informed consent was provided by patients ahead of study screening. Consent for publication: Not applicable. Competing interests: FVdB has received speaker and/or consulting fees from AbbVie, Amgen, Galapagos, Janssen, Lilly, Merck, Novartis, Pfizer, and UCB Pharma. AD has received grant/research support from AbbVie, BMS, Celgene, Lilly, MoonLake, Novartis, Pfizer, and UCB Pharma; and honoraria or consultation fees from AbbVie, BMS, Janssen, Lilly, Novartis, Pfizer, and UCB Pharma. DP has received research support from AbbVie, Lilly, MSD, Novartis, and Pfizer; and consulting fees, speaking fees, and/or honoraria from AbbVie, Biocad, BMS, Galapagos, Gilead, GSK, Janssen, Lilly, MSD, Medscape, MoonLake, Novartis, Peervoice, Pfizer, Roche, Samsung Bioepis, and UCB Pharma. WPM has received grant/research support from AbbVie, Novartis, Pfizer, and UCB Pharma; consulting fees, speaking fees, and/or honoraria fees from AbbVie, BMS, Celgene, Galapagos, Gilead, Janssen, Lilly, Medscape, Novartis, Peervoice, Pfizer, and UCB Pharma; is Chief Medical Officer of CARE Arthritis Limited; and has received royalties or licenses from Augurex for the 14-3-3eta diagnostic biomarker. DvdH has received consulting fees from AbbVie, ArgenX, BMS, Galapagos, GSK, Janssen, Lilly, Novartis, Pfizer, Takeda, and UCB Pharma; and is an editorial board member of the Journal of Rheumatology, an editorial board member of RMD Open, an associate editor for the Annals of Rheumatic Diseases, an advisor for the Assessment of Axial Spondyloarthritis International Society, and the Director of Imaging Rheumatology BV. T-HK has received speaker fees from AbbVie, Celltrion, Kirin, Lilly, and Novartis. MK has received consulting fees and/or honoraria from AbbVie, Amgen, Asahi-Kasei Pharma, Astellas, Ayumi Pharma, BMS, Chugai, Daiichi Sankyo, Eisai, Gilead, Janssen, Lilly, Novartis, Ono Pharma, Pfizer, Tanabe-Mitsubishi, and UCB Pharma. XeB has received grant/research support from AbbVie and Novartis; consulting fees from AbbVie, BMS, Chugai, MSD, Novartis, Pfizer, and UCB Pharma; speakers’ bureau fees from AbbVie, BMS, Celgene, Chugai, Merck, Novartis, Pfizer, and UCB Pharma; is an editorial board member of the Annals of Rheumatic Diseases; is the ASAS President; and is the EULAR President-elect. XiB, IL-G, I-HS, PW, KK, and AS are employees of AbbVie and may own stock or options.
Figures
References
-
- Navarro-Compan V, Sepriano A, El-Zorkany B, van der Heijde D. Axial spondyloarthritis. Ann Rheum Dis. 2021;80(12):1511–21. - PubMed
-
- Ramiro S, Nikiphorou E, Sepriano A, Ortolan A, Webers C, Baraliakos X, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. 2023;82(1):19–34. - PubMed
-
- Deodhar A, Van den Bosch F, Poddubnyy D, Maksymowych WP, van der Heidje D, Kim TH, et al. Upadacitinib for the treatment of active non-radiographic axial spondyloarthritis (SELECT-AXIS 2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2022;400(10349):369–79. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
