

Clinical subtypes in critically ill patients with sepsis: validation and parsimonious classifier model development
- PMID: 39905513
- PMCID: PMC11796029
- DOI: 10.1186/s13054-025-05256-3
Clinical subtypes in critically ill patients with sepsis: validation and parsimonious classifier model development
Abstract
Background: The application of sepsis subtypes to enhance personalized medicine in critically ill patients is hindered by the lack of validation across diverse cohorts and the absence of a simple classification model. We aimed to validate the previously identified SENECA clinical sepsis subtypes in multiple large ICU cohorts, and to develop parsimonious classifier models for δ-type adjudication in clinical practice.
Methods: Data from four cohorts between 2008 and 2023 were used to assign α, β, γ and δ-type in patients fulfilling the Sepsis-3 criteria using clinical variables: (I) The Molecular diAgnosis and Risk stratification of Sepsis (MARS, n = 2449), (II) a contemporary continuation of the MARS study (MARS2, n = 2445) (III) the Dutch National Intensive Care Evaluation registry (NICE, n = 28,621) and (IV) the Medical Information Mart for Intensive Care including (MIMIC-IV, n = 18,661). K-means clustering using clinical variables was conducted to assess the optimal number of classes and compared to the SENECA subtypes. Parsimonious models were built in the SENECA derivation cohort to predict subtype membership using logistic regression, and validated in MARS and MIMIC-IV.
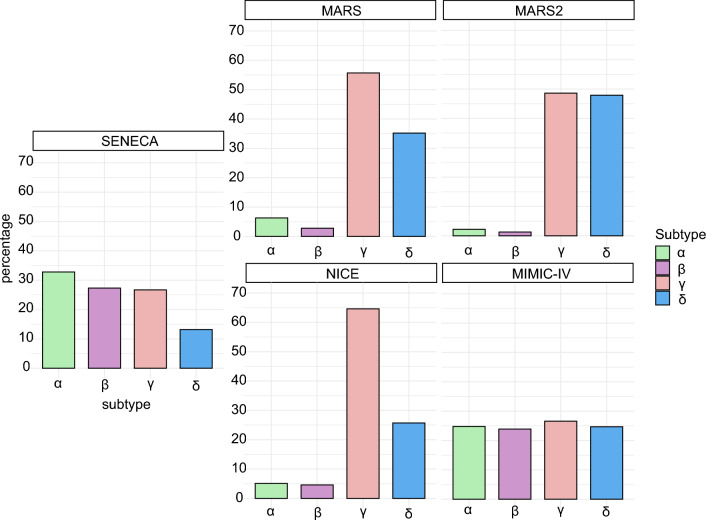
Results: Among 52.226 patients with sepsis, the subtype distribution in MARS, MARS2 and NICE was 2-6% for the α-type, 1-5% for the β-type, 49-65% for the γ-type and 26-48% for the δ-type compared to 33%, 27%, 27% and 13% in the original SENECA derivation cohort, whereas subtype distribution in MIMIC-IV was more similar at 25%, 24%, 27% and 25%, respectively. In-hospital mortality rates were significantly different between the four cohorts for α, γ and δ-type (p < 0.001). Method-based validation showed moderate overlap with the original subtypes in both MARS and MIMIC-IV. A parsimonious model for all four subtypes had moderate to low accuracy (accuracy 62.2%), while a parsimonious classifier model with 3 variables (aspartate aminotransferase, serum lactate, and bicarbonate) had excellent accuracy in predicting the δ-type patients from all other types in the derivation cohort and moderate accuracy in the validation cohorts (MARS: area under the receiver operator characteristic curve (AUC) 0.93, 95% CI [0.92-0.94], accuracy 85.5% [84.0-86.8%]; MIMIC-IV: AUC 0.86 [0.85-0.87], accuracy 82.9% [82.4-83.4%]).
Conclusions: The distribution and mortality rates of clinical sepsis subtypes varied between US and European cohorts. A three-variable model could accurately identify the δ-type sepsis patients.
Keywords: Critical illness; Machine learning; Phenotype; Precision medicine; Sepsis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: For the MARS cohorts, patients were included via an opt-out consent method approved by the institutional review boards of both participating hospitals ((Academic Medical Center in Amsterdam and University Medical Center in Utrecht) (IRB No. 10-056C). For MIMIC-IV, the institutional reviews board at the Beth Israel Deaconess Medical Center granted a waiver of informed consent and approved the data sharing initiative. Consent for publication: Not applicable. Competing interests: Hessel Peter-Sengers reports funding from the Dutch Kidney Foundation (postdoc grant 19OK009). Olaf L Cremer reports funding from ZonMw, Health Holland, and Fund SGS; research support from Abionic SA, Prolira BV, and Presymptom Health Ltd; and consulting fees from ICRC. Lieuwe DJ Bos reports support from the Dutch Lung Foundation (Young Investigator Grant and Dirkje Postma Award), the Dutch Lung Foundation and Health Holland (Grant Public–Private Partnership), the IMI COVID19 initiative, Amsterdam UMC, ZonMW (COVID-19 Urgency Grant and VIDI Grant), the ERS Gold Metal for ARDS and unrestricted research grants from Santhera and Volition; consulting fees for Scailyte, Sobi, Exvastat, Santhera, Pfizer, Astra Zeneca, and Janssen paid to the institution. Alexander PJ Vlaar reports support by a Landsteiner Foundation for Blood Research (LSBR) fellowship grant, number 1931F. from the Landsteiner Foundation for Blood Transfusion Research, Haarlem – The Netherlands and by a personal grant of NWO (VIDI Grant number 09150172010047); and consulting fees from Edwards Lifesciences, CSL Behringe, InflaRx paid to the institution; and grants from Edwards Lifesciences, CSL Behringe, Terumo and Werfen. Jason N Kennedy and Christopher W Seymour were supported by the National Institutes of Health grant R35GM119519. Lonneke A van Vught was supported by the Netherlands Organisation for Health Research and Development ZonMW (Nederlandse Organisatie voor Wetenschappelijk Onderzoek NWO) VENI grant 09150161910033 and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Research Grant.
Figures
References
-
- Vincent JL, Marshall JC, Namendys-Silva SA, Francois B, Martin-Loeches I, Lipman J, et al. Assessment of the worldwide burden of critical illness: the Intensive Care Over Nations (ICON) audit. Lancet Respir Med. 2014;2(5):380–6. - PubMed
-
- Cohen J, Vincent JL, Adhikari NK, Machado FR, Angus DC, Calandra T, et al. Sepsis: a roadmap for future research. Lancet Infect Dis. 2015;15(5):581–614. - PubMed
-
- Marshall JC. Why have clinical trials in sepsis failed? Trends Mol Med. 2014;20(4):195–203. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
