

Length of stay after colorectal surgery in Italy: the gap between "fit for" and "actual" discharge in a prospective cohort of 4529 cases
- PMID: 39905571
- PMCID: PMC11796130
- DOI: 10.1186/s13741-025-00492-1
Length of stay after colorectal surgery in Italy: the gap between "fit for" and "actual" discharge in a prospective cohort of 4529 cases
Abstract
Background: It is common to observe a gap between the day on which the discharge criteria are reached and the actual day of discharge after colorectal surgery. The aim of this study is to understand the reasons for this difference and its clinical impact on the overall length of stay (LOS).
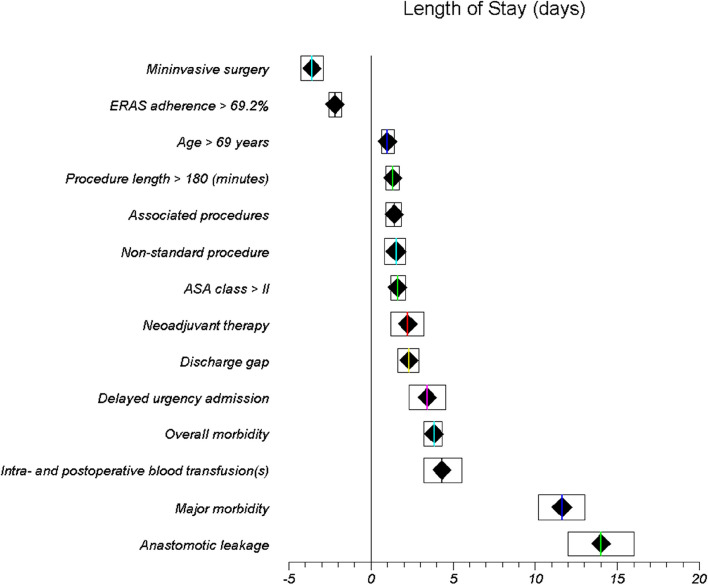
Methods: All patients enrolled in the prospective iCral3 study were analyzed regarding any difference and reason between the "fit for discharge" (FFD) and "actual discharge" (AD) dates. The association between the gap and the LOS in the whole population was then assessed through a multivariate regression model including other confounding variables.
Results: The analysis included 4529 patients, with a median [IQR] LOS of 6 [4-8] days. The median [IQR] LOS was 6 [4-8] days in the no-gap group (3,910 patients, 86.3%), significantly lower (p < .001) than 7 [6-10] days in the gap group (619 patients, 13.7%). Among the gap reasons, the "need for postoperative rehabilitation" compared to "not willing to return home" and "social constraints" was associated with the longest LOS (9 [6.0-12.5] days, p < 0.001 vs other reasons). The existence of the gap independently determined a 2.3-day lengthening of LOS.
Conclusions: Among other factors, the gap between FFD and AD had an independent impact on LOS. The most frequent reasons for this gap were "not willing to return home" and "social constraint", while the "need for postoperative rehabilitation" had the greater clinical impact.
Keywords: Actual discharge; Colorectal surgery; ERAS; Fit for discharge; Length of stay.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki and the Guideline for Good Clinical Practice E6 (R2) principles. The study protocol was approved by the coordinating center ethics committee (Comitato Etico Regionale delle Marche–C.E.R.M. #2020/192, approved on 07/30/2020) and registered at ClinicalTrials.gov (NCT04397627). Thereafter, all participating centers obtained authorization from the local institutional review board. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for cohort studies. Individual participant-level anonymized datasets were made available upon reasonable request by contacting the study coordinator. Informed consent was obtained from all individual participants included in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Agenzia Nazionale per i Servizi Sanitari Regionali (AGENAS), Programma Nazionale Esiti (PNE) edizione 2023, accessed online on July 10, 2024.
-
- Balvardi S, Pecorelli N, Castelino T, Niculiseanu P, Liberman AS, Charlebois P, Stein B, Carli F, Mayo NE, Feldman LS, Fiore JF Jr. Measuring in-hospital recovery after colorectal surgery within a well-established enhanced recovery pathway: a comparison between hospital length of stay and time to readiness for discharge. Dis Colon Rectum. 2018;61(7):854–60. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
