

Rapid diagnostic testing combined with an immediate infectious disease consultation increases the rate of septic intensive care unit patients on targeted antibiotic therapy
- PMID: 39906215
- PMCID: PMC11790461
- DOI: 10.3389/fcimb.2024.1513408
Rapid diagnostic testing combined with an immediate infectious disease consultation increases the rate of septic intensive care unit patients on targeted antibiotic therapy
Abstract
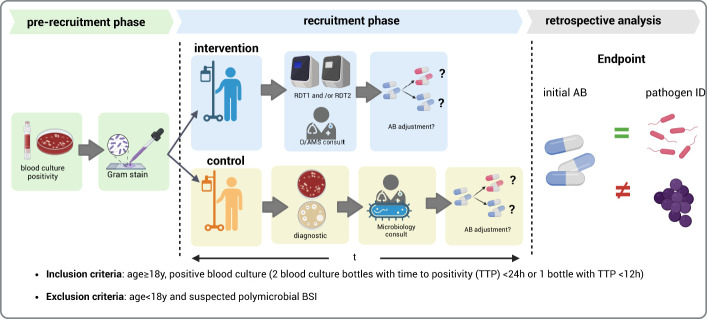
Objectives: To evaluate the impact of rapid diagnostic testing (RDT) combined with immediate infectious disease (ID) consultation on the treatment of septic patients with positive blood cultures in intensive care units in a setting without 24/7 service.
Methods: Adult ICU patients in a tertiary care hospital with positive blood cultures were included from January 2019 to December 2020. The control group underwent routine laboratory testing, and for the intervention group, RDT was applied with immediate ID consultation.
Results: In 77 out of the 91 patients in the intervention group, the pathogen was identified by RDT. Regarding antimicrobial susceptibility testing (AST), genotypic testing (ePlex®) was successful for Gram-positive cocci, but inadequate for Gram-negative rods. Phenotypic resistance testing with the Accelerate PhenoTest® took too long to be successfully integrated into the intervention. Adaptation of empirical antibiotic therapy was recommended for 72.7% of the patients. Adherence to the ID consultation post-RDT results was high at 82.3%. In the control group, adaptation of the initial antibiotic therapy would have been recommended for 81.8% of patients, if the species identification had been available. Overall adherence to the local antibiotic therapy guideline for sepsis was significantly lower in the control than in the intervention group (27.8% versus 89.3%, p<0.001).
Conclusion: Integration of an RDT system in the microbiological workflow for septic patients in ICU combined with a standardized ID intervention led to a significantly higher percentage of adequate antimicrobial treatment and greater adherence to local antibiotic therapy recommendations, even in a setting where 24/7 service is not available.
Keywords: adequate antibiotic therapy; antimicrobial stewardship (AMS); blood stream infection (BSI); infectious diseases consultation; rapid diagnostic testing; sepsis.
Copyright © 2025 Kramme, Käding, Graf, Schmoll, Linnen, Nagel, Grote-Levi, Hauswaldt, Nurjadi and Rupp.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The real-world impact of the BioFire FilmArray blood culture identification 2 panel on antimicrobial stewardship among patients with bloodstream infections in intensive care units with a high burden of drug-resistant pathogens.J Microbiol Immunol Infect. 2024 Aug;57(4):580-593. doi: 10.1016/j.jmii.2024.06.004. Epub 2024 Jun 20. J Microbiol Immunol Infect. 2024. PMID: 38942661
-
A Role for Antimicrobial Stewardship in Clinical Sepsis Pathways: a Prospective Interventional Study.Infect Control Hosp Epidemiol. 2017 Sep;38(9):1032-1038. doi: 10.1017/ice.2017.139. Epub 2017 Jul 11. Infect Control Hosp Epidemiol. 2017. PMID: 28693625
-
Rapid and cost-effective identification and antimicrobial susceptibility testing in patients with Gram-negative bacteremia directly from blood-culture fluid.J Microbiol Methods. 2018 Mar;146:7-12. doi: 10.1016/j.mimet.2018.01.012. Epub 2018 Feb 3. J Microbiol Methods. 2018. PMID: 29366760
-
[Bacterial sepsis : Diagnostics and calculated antibiotic therapy].Anaesthesist. 2017 Oct;66(10):737-761. doi: 10.1007/s00101-017-0363-8. Anaesthesist. 2017. PMID: 28980026 Review. German.
-
Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection.Cochrane Database Syst Rev. 2021 May 4;5(5):CD013235. doi: 10.1002/14651858.CD013235.pub2. Cochrane Database Syst Rev. 2021. PMID: 34097767 Free PMC article.
Cited by
-
Antibiotic De-Escalation in the Intensive Care Unit: Rationale and Potential Strategies.Antibiotics (Basel). 2025 May 3;14(5):467. doi: 10.3390/antibiotics14050467. Antibiotics (Basel). 2025. PMID: 40426534 Free PMC article. Review.
References
-
- Banerjee R., Teng C. B., Cunningham S. A., Ihde S. M., Steckelberg J. M., Moriarty J. P., et al. . (2015). Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin. Infect. Dis. 61, 1071–1080. doi: 10.1093/cid/civ447 - DOI - PMC - PubMed
-
- Britt N. S., Khader K., He T., Willson T. M., Effiong A., Timbrook T. T., et al. . (2023). Examining the clinical impact of rapid multiplex polymerase chain reaction-based diagnostic testing for bloodstream infections in a national cohort of the Veterans Health Administration. Pharmacotherapy 43, 24–34. doi: 10.1002/phar.2747 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical