

Exploring the potential mediating role of systemic antibiotics in the association between early-life lower respiratory tract infections and asthma at age 5 in the CHILD study
- PMID: 39906720
- PMCID: PMC11790586
- DOI: 10.3389/falgy.2024.1463867
Exploring the potential mediating role of systemic antibiotics in the association between early-life lower respiratory tract infections and asthma at age 5 in the CHILD study
Abstract
Objective: Lower respiratory tract infections (LRTIs) in early life are one of the strongest risk factors for childhood asthma and are often treated with systemic antibiotics (IV or oral). We aimed to explore the association between early-life LRTIs and systemic antibiotics on asthma development and the potential mediating role of antibiotics in this relationship.
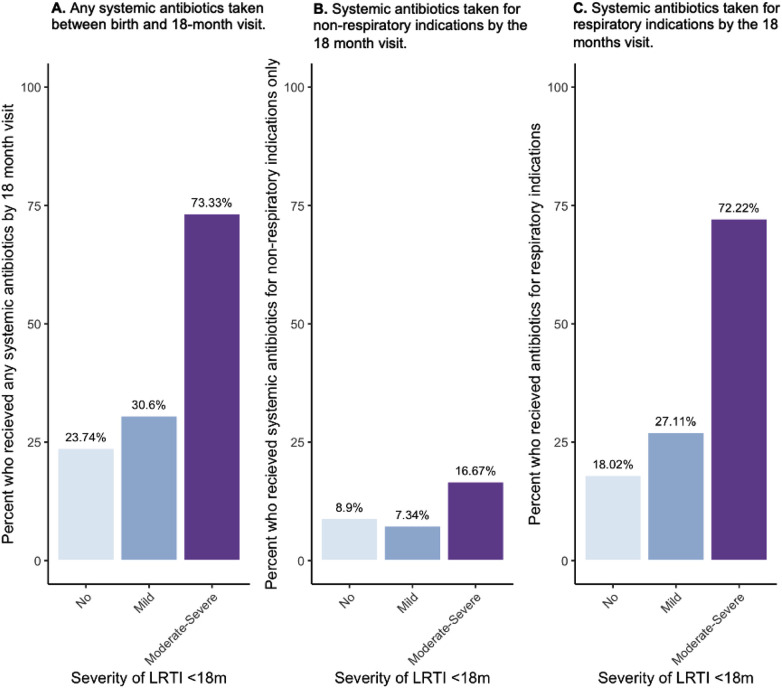
Methods: Data were collected as part of the longitudinal, general Canadian population CHILD Study. LRTIs during the first 18 months of life were identified through parental symptom report at regular study visits. Systemic antibiotic use was defined as at least one dose of oral/intravenous antibiotics between birth and the 18-month visit and were further categorized by indication as either given for a respiratory indication (upper or lower respiratory symptoms) or non-respiratory indication. Asthma was diagnosed by in-study pediatricians at the 5-year study visit. Adjusted logistic regression models and mediation analyses via systemic antibiotics use were performed.
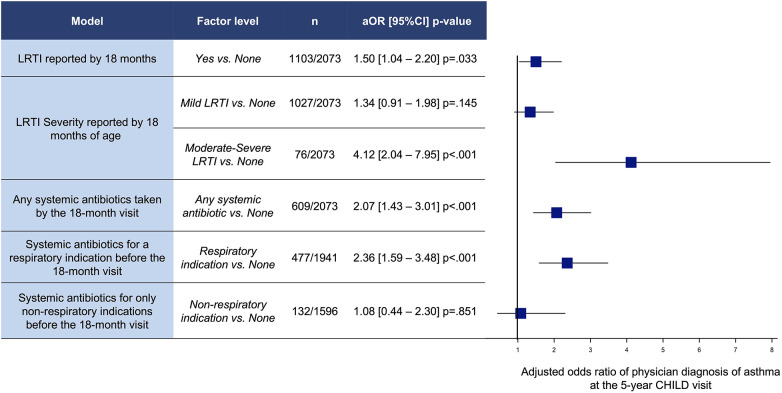
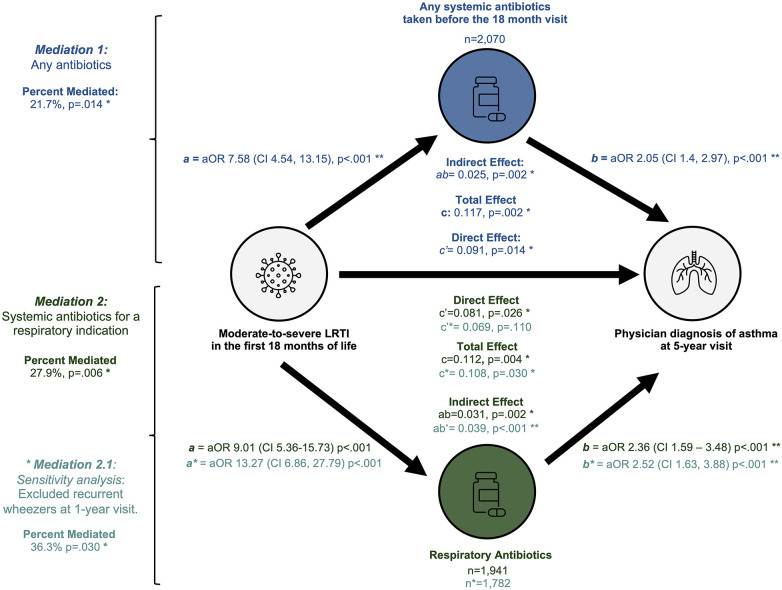
Results: Among 2,073 participants included in our analysis, 72 (4.9%) had asthma age 5, and 609 (29.3%) used systemic antibiotics before the 18-month visit. Among children who had taken antibiotics, 61.6% also had an LRTI in that period compared to 49.7% among children without exposure to systemic antibiotics (p < .001). Moderate-severe LRTIs before age 18 months were associated with higher odds of 5-year asthma [aOR 4.12 (95%CI 2.04-7.95) p < .001]. Antibiotics taken for respiratory indications were associated with higher odds of asthma at age 5 [aOR 2.36 (95%CI 1.59-3.48) p < .001]. Children who received systemic antibiotics for only non-respiratory indications during the first 18 months of life were not associated with increased odds of asthma [aOR 1.08 (95%CI 0.44-2.30) p = .851]. Using mediation analysis, 21.7% of the association between LRTI and asthma is estimated to be mediated through use of early-life systemic antibiotics. However, a significant direct effect of moderate-to-severe LRTIs on asthma risk remained in adjusted mediation models (p = .014).
Conclusion: Through mediation modeling we estimate that the increased risk of asthma at age 5 that is associated with moderate-severe LRTIs in infancy may be partially mediated by systemic antibiotics taken during the first 18 months of life. This underscores the importance of public health strategies focused on antibiotic stewardship and reducing early life LRTIs to mitigate asthma risk.
Keywords: antibiotics; clinical epidemiology; cohort study; mediation analyses; preschool asthma; respiratory tract infections.
© 2025 Medeleanu, Reyna, Dai, Winsor, Brinkman, Verma, Nugent, Riaz, Simons, Mandhane, Azad, Turvey, Moraes and Subbarao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Asthma occurrence in children and early life systemic antibiotic use: an incidence density study.Allergy Asthma Clin Immunol. 2023 Mar 6;19(1):18. doi: 10.1186/s13223-023-00773-8. Allergy Asthma Clin Immunol. 2023. PMID: 36879341 Free PMC article.
-
Early childhood respiratory tract infections according to parental subfertility and conception by assisted reproductive technologies.Hum Reprod. 2022 Aug 25;37(9):2113-2125. doi: 10.1093/humrep/deac162. Hum Reprod. 2022. PMID: 35881052 Free PMC article.
-
Moderate-to-severe lower respiratory tract infection in early life is associated with increased risk of polysensitization and atopic dermatitis: Findings from the CHILD Study.J Allergy Clin Immunol Glob. 2022 Jan 17;1(2):73-79. doi: 10.1016/j.jacig.2021.12.005. eCollection 2022 May. J Allergy Clin Immunol Glob. 2022. PMID: 37780586 Free PMC article.
-
Clinical recommendations for the inpatient management of lower respiratory tract infections in children and adolescents with severe neurological impairment in Germany.Eur J Pediatr. 2024 Mar;183(3):987-999. doi: 10.1007/s00431-023-05401-6. Epub 2024 Jan 3. Eur J Pediatr. 2024. PMID: 38172444 Free PMC article. Review.
-
Antibiotic strategies for eradicating Pseudomonas aeruginosa in people with cystic fibrosis.Cochrane Database Syst Rev. 2023 Jun 2;6(6):CD004197. doi: 10.1002/14651858.CD004197.pub6. Cochrane Database Syst Rev. 2023. PMID: 37268599 Free PMC article. Review.
References
-
- Global Asthma Network. The Global Asthma Report 2022. Wisconsin: The GINA Scientific Committee (2022). Available online at: http://www.globalasthmareport.org/ (Accessed December 14, 2023).
LinkOut - more resources
Full Text Sources