

Efficacy and safety of premixed versus basal-bolus regimens as intensification of insulin therapy in patients with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized clinical trials
- PMID: 39907628
- PMCID: PMC12057386
- DOI: 10.1111/jdi.70002
Efficacy and safety of premixed versus basal-bolus regimens as intensification of insulin therapy in patients with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized clinical trials
Abstract
Aim: To estimate the efficacy and safety of the basal-bolus and premixed insulin as intensification regimens in patients with type 2 diabetes mellitus (T2DM).
Methods: A comprehensive search of online databases was performed until December 2022 to identify randomized controlled trials (RCTs) comparing premixed insulin versus basal-bolus regimen with treat-to-target intention. The Cochrane ROB-2 tool and GRADE approach were used for quality assessment and certainty of the evidence, respectively. Pooled weighted mean difference (WMD) and odds ratio (OR) were calculated using random-effects meta-analysis models.
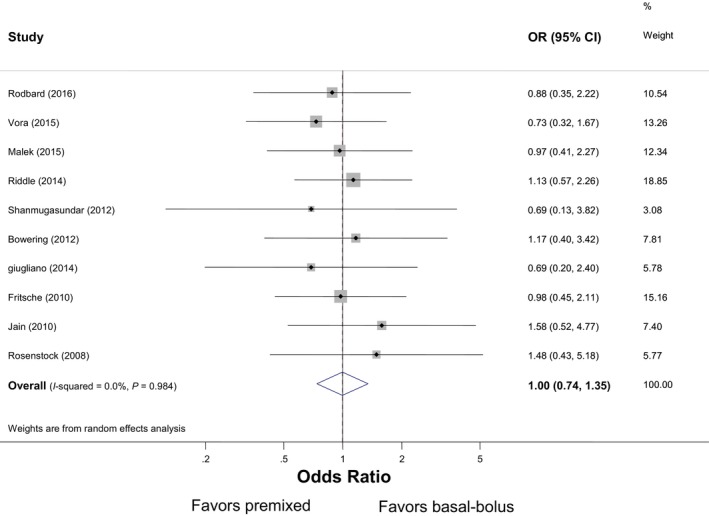
Results: Eighteen RCTs were included in the meta-analysis, and 66% had a low risk of bias. We found no significant difference between the two regimens regarding HbA1c reduction (WMD: 0.03% [-0.05%, 0.10%]). The basal-bolus regimen improved fasting plasma glucose (FPG) more than the premixed regimen (WMD: 6.35 mg/dL [0.31, 12.39]). Both had similar effects on weight gain. The odds of developing overall, nocturnal, and severe hypoglycemia were comparable (pooled OR: 0.9, 1.02, and 1.00, respectively) with no heterogeneity. Findings of the model were robust. The certainty of the evidence was moderate to high for all outcomes except FPG.
Conclusions: Two regimens are clinically comparable. Patient preference should be considered when adopting an individualized approach in a real-world setting.
Keywords: Basal‐bolus Insulin; Premixed Insulin; Type 2 Diabetes Mellitus.
© 2025 The Author(s). Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Figures






Similar articles
-
Personalized intensification of insulin therapy in type 2 diabetes - does a basal-bolus regimen suit all patients?Curr Med Res Opin. 2016 Aug;32(8):1425-34. doi: 10.1080/03007995.2016.1181051. Epub 2016 May 25. Curr Med Res Opin. 2016. PMID: 27126277 Review.
-
Premixed vs basal-bolus insulin regimen in Type 2 diabetes: comparison of clinical outcomes from randomized controlled trials and real-world data.Diabet Med. 2017 Dec;34(12):1728-1736. doi: 10.1111/dme.13518. Epub 2017 Oct 14. Diabet Med. 2017. PMID: 28945928
-
Randomized, open-label, parallel-group evaluations of basal-bolus therapy versus insulin lispro premixed therapy in patients with type 2 diabetes mellitus failing to achieve control with starter insulin treatment and continuing oral antihyperglycemic drugs: a noninferiority intensification substudy of the DURABLE trial.Clin Ther. 2010 May;32(5):896-908. doi: 10.1016/j.clinthera.2010.05.001. Clin Ther. 2010. PMID: 20685497 Clinical Trial.
-
Sliding scale insulin for non-critically ill hospitalised adults with diabetes mellitus.Cochrane Database Syst Rev. 2018 Nov 29;11(11):CD011296. doi: 10.1002/14651858.CD011296.pub2. Cochrane Database Syst Rev. 2018. PMID: 30488948 Free PMC article.
-
Comparison of thrice-daily premixed insulin (insulin lispro premix) with basal-bolus (insulin glargine once-daily plus thrice-daily prandial insulin lispro) therapy in east Asian patients with type 2 diabetes insufficiently controlled with twice-daily premixed insulin: an open-label, randomised, controlled trial.Lancet Diabetes Endocrinol. 2015 Apr;3(4):254-62. doi: 10.1016/S2213-8587(15)00041-8. Epub 2015 Mar 6. Lancet Diabetes Endocrinol. 2015. PMID: 25754414 Clinical Trial.
References
-
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas. Diabetes Res Clin Pract 2019; 157: 107843. - PubMed
-
- American Diabetes Association 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes‐2021. Diabetes Care 2021; 44(Suppl 1): S15–S33. - PubMed
-
- American Diabetes Association Professional Practice Committee: 9. Pharmacologic approaches to glycemic treatment: Standards of medical care in diabetes‐2022. Diabetes Care 2022; 45: S125–S143. - PubMed
-
- Baena‐Díez JM, Penafiel J, Subirana I, et al. Risk of cause‐specific death in individuals with diabetes: A competing risks analysis. Diabetes Care 2016; 39: 1987–1995. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
