

Nurses' Perspectives and Experiences of Using a Bed-Exit Information System in an Acute Hospital Setting: Mixed Methods Study
- PMID: 39908092
- PMCID: PMC11840387
- DOI: 10.2196/64444
Nurses' Perspectives and Experiences of Using a Bed-Exit Information System in an Acute Hospital Setting: Mixed Methods Study
Abstract
Background: Technology that detects early when a patient at risk of falling leaves the bed can support nurses in acute care hospitals.
Objective: To develop a better understanding of nurses' perspectives and experiences with a bed-exit information system (BES) in an acute care hospital setting.
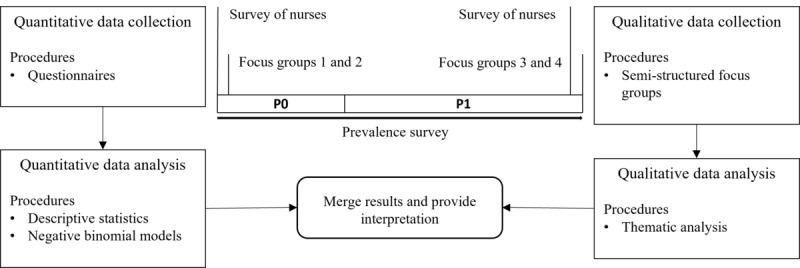
Methods: BES was implemented on 3 wards of a university medical center. Nurses completed 2 online surveys at each time point (P0 and P1) and participated in focus groups before (P0) and after (P1) implementation. Additional patient data were collected. Descriptive statistics summarized the survey results, while content analysis was applied to focus group data. Patient rates and adverse events in both phases were compared using negative binomial models. Reporting of this study adhered to the GRAMMS checklist.
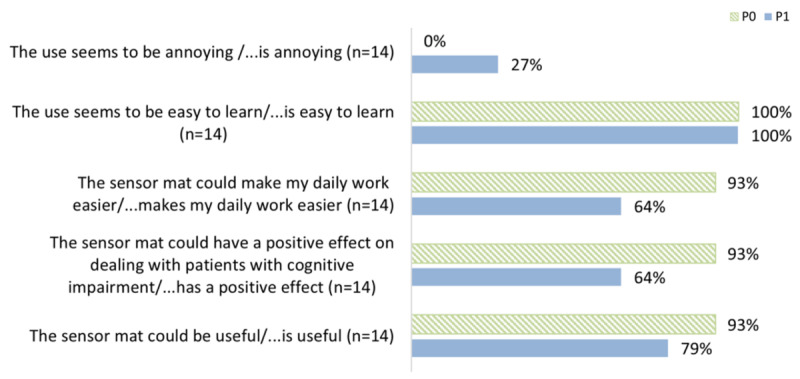
Results: A total of 30 questionnaires were completed at P0 (30/72, 42%) and 24 at P1 (24/71, 33%). Of the participants, 15 completed both questionnaires (complete cases). At P1, 64% (9/14) of participants agreed that their perceived workload and strain in caring for patients with cognitive impairment was reduced by the use of the BES. The adverse event rate per patient per day was reduced by a factor of 0.61 (95% CI 0.393-0.955; P=.03). In addition, 11 nurses participated in 4 focus groups before and after the intervention. Participants found it challenging to operationalize the use of the BES due to the heterogeneity of care settings, but certain behaviors of patients with cognitive impairment were recognized as indicating a need for intervention. Negative experiences included information overload and alarm fatigue, leading to occasional removal of the system.
Conclusions: While BES provides some support in managing patients with cognitive impairment, its impact remains limited to specific scenarios and does not significantly reduce nurses' workload or strain. Our findings highlight the need to manage expectations of BES performance to ensure alignment between expected and actual benefits. To improve BES effectiveness and long-term implementation, future research should consider both objective measures of patient care and subjective factors such as nurse experience, structural conditions, and technical specifications. Improving information mechanisms within call systems could help reduce alarm fatigue and increase perceived usefulness. Overall, successful integration of BES in acute care settings will require close collaboration with nursing staff to drive meaningful healthcare innovation and ensure that the technology meets the needs of both patients and nurses.
Trial registration: German Register for Clinical Studies DRKS00021720; https://drks.de/search/de/trial/DRKS00021720.
Keywords: acute hospital; bed-exit; cognitive impairment; cognitively impaired; fall prevention; hospital; information system; inpatient; mixed methods; nurse; online questionnaire; support; technology; workload.
©Stefan Walzer, Isabel Schön, Johanna Pfeil, Sam Klemm, Sven Ziegler, Claudia Schmoor, Christophe Kunze. Originally published in JMIR Formative Research (https://formative.jmir.org), 05.02.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Fogg C, Griffiths P, Meredith P, Bridges J. Hospital outcomes of older people with cognitive impairment: an integrative review. Int J Geriatr Psychiatry. 2018;33(9):1177–1197. doi: 10.1002/gps.4919. https://europepmc.org/abstract/MED/29947150 - DOI - PMC - PubMed
-
- Motzek T, Büter K, Mächler K, Junge M, Marquardt G. Orientierungsschwierigkeiten, behaviorale und psychiatrische Symptome bei patienten mit kognitiven Einschränkungen im Krankenhaus. HBScience. 2017;8(2):46–51. doi: 10.1007/s16024-017-0297-8. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
