

Allogeneic off-the-shelf CAR T-cell therapy for relapsed or refractory B-cell malignancies
- PMID: 39908482
- PMCID: PMC11995077
- DOI: 10.1182/bloodadvances.2024015157
Allogeneic off-the-shelf CAR T-cell therapy for relapsed or refractory B-cell malignancies
Abstract
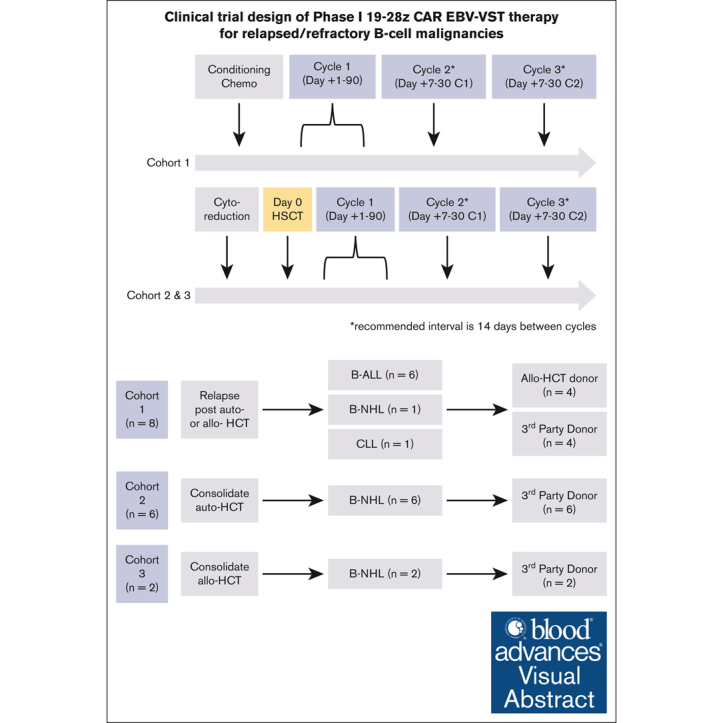
Despite clinical benefit with the use of chimeric antigen receptor (CAR) T cells, the need to manufacture patient-specific products limits its clinical utility. To overcome this barrier, we developed an allogeneic "off-the-shelf" CAR T-cell product using Epstein-Barr virus (EBV)-specific T cells (EBV-VSTs) genetically modified with a CD19-specific CAR (19-28z). Patients with relapsed/refractory (R/R) B-cell malignancies were stratified into 3 treatment cohorts: cohort 1 (n = 8; disease recurrence after allogeneic or autologous hematopoietic cell transplantation [HCT]), cohort 2 (n = 6; consolidative therapy after autologous HCT), or cohort 3 (n = 2; consolidative therapy after allogeneic HCT). The primary objective of this trial was to determine the safety of multiple CAR EBV-VST infusions. Most patients (n = 12/16) received multiple doses (overall median, 2.5 [range, 1-3]) with 3 × 106 T cells per kg determined to be the optimal dose enabling multiple treatments per manufactured cell line. Severe cytokine release syndrome or neurotoxicity did not occur after infusion, and no dose-limiting toxicity was observed in the trial. Median follow-up was 48 months (range, 4-135) with 4 deaths due to disease progression. Overall survival of all patients was 81% at 12 months and 75% at 36 months. Postinfusion expansion and persistence were limited, and CAR EBV-VSTs demonstrated a unique T-cell phenotype compared with autologous 19-28z CAR T cells. Our study demonstrates the feasibility and safety of an allogeneic "off-the-shelf" CAR EBV-VST product with favorable outcomes for patients with CD19+ R/R B-cell malignancies. This trial was registered at www.ClinicalTrials.gov as #NCT01430390.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: K.J.C. has received research support from Atara Biotherapeutics, Novartis, Celgene, and Cellectis, and has consulted and participated in advisory boards for Novartis. S.E.P. has received support for the conduct of clinical trials through Boston Children’s Hospital from AlloVir, Atara Biotherapeutics, and Jasper; is the inventor of intellectual property related to development of third-party viral-specific T-cell program, with all rights assigned to Memorial Sloan Kettering Cancer Center; and reports honoraria, consulting, or participation in advisory board for Pierre Fabre, Regeneron, Cellevolve, Vor, and Ensomo, DSMB, Stanford University, and New York Blood Center. J.J.B. has consulted for Merck, Sanofi, Sobi, and SmartImmune and received compensation for serving on data monitoring committee DMC (either chair or member) for Advanced Clinical and CTI Clinical Trial Services. N.A.K. holds equity in Amgen, Johnson & Johnson, and Merck. R.B. has licensed intellectual property to and collects royalties from Bristol Myers Squibb (BMS), Caribou, and Sanofi; received research funding from BMS; is a consultant to BMS and Atara Biotherapeutics Inc; and was on the scientific advisory board of Triumvira, Cargo Tx, and CoImmune. R.J.O. received royalties, research support, and consulting from Atara Biotherapeutics. M.S. reports research support from Atara Biotherapeutics and has licensed intellectual property to Juno Therapeutics, Atara Biotherapeutics, Fate Therapeutics, Takeda Pharmaceuticals, Mnemo Therapeutics, and Minerva Biotechnologies. I.R. is a scientific cofounder of Mnemo Therapeutics and reports participation in the advisory board of Center for Commercialization of Cancer.
Figures





References
-
- Fielding AK, Richards SM, Chopra R, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109(3):944–950. - PubMed
-
- von Stackelberg A, Völzke E, Kühl JS, et al. Outcome of children and adolescents with relapsed acute lymphoblastic leukaemia and non-response to salvage protocol therapy: a retrospective analysis of the ALL-REZ BFM Study Group. Eur J Cancer. 2011;47(1):90–97. - PubMed
-
- Tachibana T, Kanda J, Ishizaki T, et al. Outcomes and prognostic factors for patients with relapsed or refractory acute lymphoblastic leukemia who underwent allogeneic hematopoietic cell transplantation: a KSGCT multicenter analysis. Biol Blood Marrow Transplant. 2020;26(5):998–1004. - PubMed
-
- Gianni AM, Berinstein NL, Evans PA, López-Guillermo A, Solano C. Stem-cell transplantation in non-Hodgkin's lymphoma: improving outcome. Anti Cancer Drugs. 2002;13(suppl 2):S35–S42. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
