

Implementation of guideline-directed medical therapy in patients with heart failure with reduced ejection fraction (OpTIMa-HF Registry)
- PMID: 39909062
- PMCID: PMC12055350
- DOI: 10.1002/ehf2.15172
Implementation of guideline-directed medical therapy in patients with heart failure with reduced ejection fraction (OpTIMa-HF Registry)
Abstract
Aims: The last released European guidelines on the management of heart failure (HF) recommend in patients with chronic HF with reduced ejection fraction (HFrEF) a pharmacological approach based on four fundamental drugs to be rapidly implemented and then uptitrated to modify disease progression. The aim of the Optimization of Therapy in the Italian Management of Heart Failure (OPTIMA-HF) registry is to collect data on chronic HF outpatients in different settings of care. In the present analysis, we report the first analysis of the OPTIMA-HF registry, focusing on the real-life use of guideline-directed medical therapy in patients affected by HFrEF.
Methods: OPTIMA-HF is an observational, cross-sectional, multicentre, real-life Italian registry conducted in two different clinical settings: HF outpatients' clinics of Italian hospitals and community HF outpatients' services. The study comprises a T0 phase-retrospective data collection, in which data of consecutive HF outpatients seen between January and October 2022 were collected; an educational activity phase; and a T1 phase-prospective data collection, in which data of consecutive HF outpatients seen between September 2023 and November 2023 were collected. In the present analysis, we describe the T0 phase focusing on HFrEF drug prescription rates, types, doses, combination therapy, the presence of contraindications and reasons of non-optimized treatment.
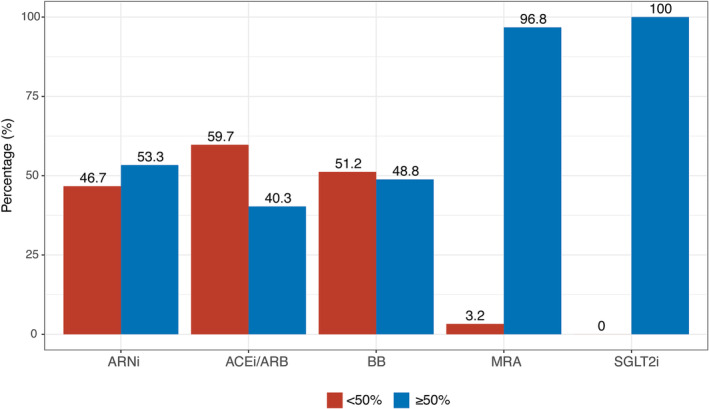
Results: Twenty-nine centres enrolled 2110 HF patients, of which 1390 (65.9%) had HFrEF [69.5 ± 11.9 years, 76.2% males, 4.1 years since HF diagnosis, median ejection fraction (EF) 33%]. Among HFrEF patients, 89.1% were on treatment with renin-angiotensin-aldosterone system inhibitor (RAASi)/angiotensin receptor neprilysin inhibitor (ARNI) (72% ARNI and 17.1% RAASi), 95.1% with beta-blockers, 75.8% with mineralocorticoid receptor antagonists (MRA) and 63.2% with sodium/glucose cotransporter 2 inhibitors (SGLT2i). Despite high prescription rates, a non-negligible number of patients with no contraindications were not treated with each specific drug. Patients taking all four drug classes, as recommended by guidelines, were mere 46.9%. Regarding doses, a still low number of patients on RAASi/ARNI and beta-blockers were treated with a dose ≥50% of the target doses recommended by the European guidelines.
Conclusions: The OPTIMA-HF registry reported that HFrEF fundamental drugs are prescribed in most Italian patients; however, <50% of patients receive optimal combination therapy, and still not a satisfying number of patients receive target doses. Strategies to improve implementation of guideline-directed medical therapy are needed to improve HF prognosis.
Keywords: HFrEF; disease‐modifying drugs; guideline‐directed medical therapy; heart failure; pharmacotherapy.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
-
- Vaduganathan M, Claggett BL, Jhund PS, Cunningham JW, Pedro Ferreira J, Zannad F, et al. Estimating lifetime benefits of comprehensive disease‐modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: a comparative analysis of three randomised controlled trials. Lancet 2020;396:121‐128. doi:10.1016/S0140-6736(20)30748-0 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
