

Diabetes beliefs, perceived risk and health behaviours: an embedded mixed-methods analysis from the Richmond Stress and Sugar Study
- PMID: 39909528
- PMCID: PMC11800224
- DOI: 10.1136/bmjopen-2024-089922
Diabetes beliefs, perceived risk and health behaviours: an embedded mixed-methods analysis from the Richmond Stress and Sugar Study
Abstract
Introduction: Efforts to increase engagement with diabetes prevention programmes largely focus on increasing diabetes awareness, with the logic that risk knowledge will motivate behaviour change. However, the salience of perceived risk as it relates to diabetes prevention is contested. The goal of this cross-sectional, embedded mixed-methods study was to examine the relationships between perceived risk, diabetes beliefs and prevention behaviours among adults at elevated risk of type 2 diabetes.
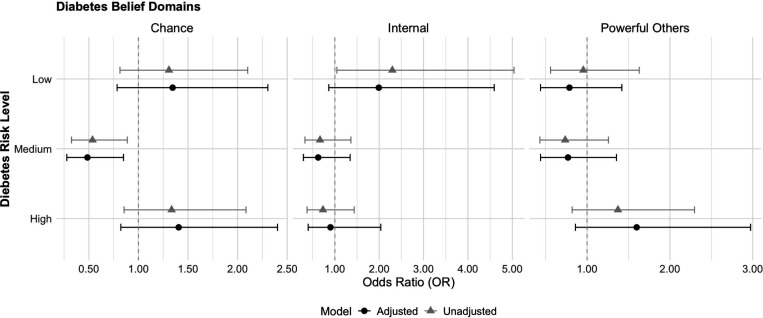
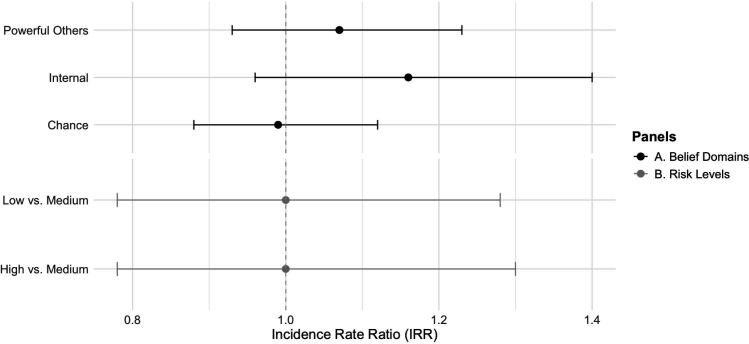
Methods: Data come from the Richmond Stress and Sugar Study (n=125). Diabetes beliefs (ie, internal, chance, powerful others) were assessed using the Multidimensional Health Locus of Control. Preventive behaviours (eg, changing diet, exercise, tobacco, alcohol) were measured by self-report. Perceived risk of developing diabetes was measured using a probability scale (0%-100%). Logistic and Poisson regression models quantified the relationships between beliefs, behaviours and perceived risk. Qualitative themes regarding challenges and facilitators to preventive behaviours were abstracted from open-ended questions and summarised using content analysis.
Results: Perceived risk of developing diabetes was low (median: 35% likelihood) and only 10% of participants had ever attended a prevention class. None of the diabetes belief domains were significantly associated with either engagement in preventive behaviours or perceived diabetes risk. Perceived diabetes risk was not associated with engagement in preventive behaviours; however, having a family history of diabetes was strongly related to perceived risk (OR: 3.35, 95% CI: 1.42 to 7.86). Qualitative facilitators and barriers of preventive behaviours reflected psychosocial factors (eg, determination, stress, preferences) and resources (eg, social support, time, overall health).
Conclusions: Perceptions of risk and health beliefs are not correlated with engagement in preventive behaviours among adults at clinically elevated risk of diabetes. Awareness campaigns may benefit from incorporating family health history information. Diabetes prevention programmes should address barriers beyond health beliefs to promote engagement in behaviour change.
Keywords: Behavior; Diabetes Mellitus, Type 2; MENTAL HEALTH.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical