

Chronic postsurgical inguinal pain: incidence and diagnostic biomarkers from a large German national claims database
- PMID: 39909798
- PMCID: PMC12106889
- DOI: 10.1016/j.bja.2024.11.048
Chronic postsurgical inguinal pain: incidence and diagnostic biomarkers from a large German national claims database
Abstract
Background: Chronic postsurgical inguinal pain (CPIP) is the most common complication of groin hernia surgery. The characteristics of patients, their medical care, and choice of diagnostic tools remain to be defined to optimise preventive and therapeutic interventions.
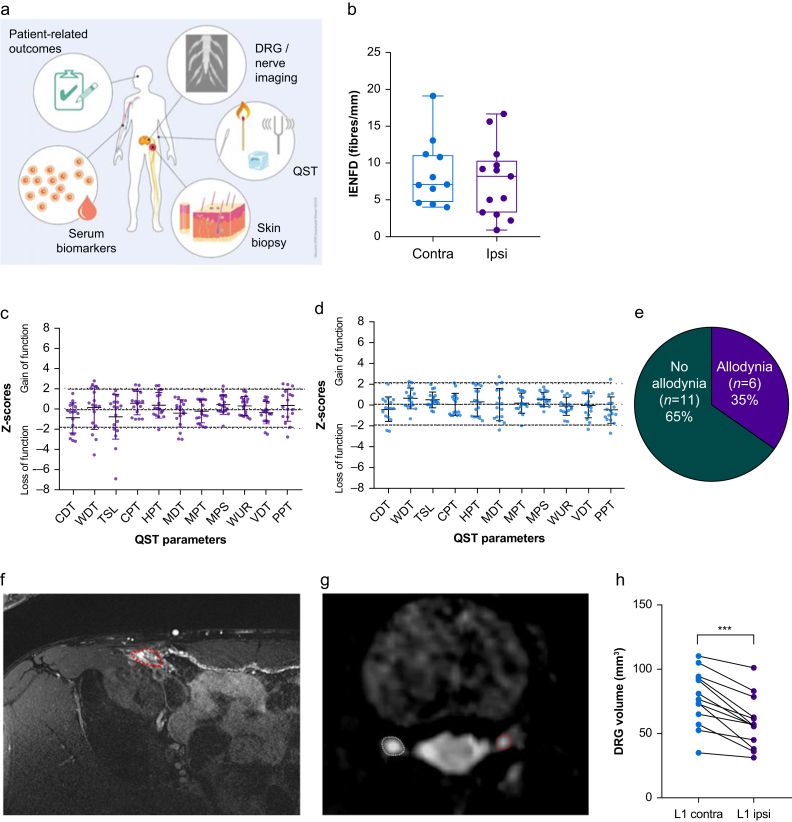
Methods: Claims data from 2018 and a 1-yr follow-up were analysed for incidence and medical care. A separate cohort (141 healthy controls and 17 CPIP patients) was examined by deep phenotyping. This included sensory testing, blood and skin biopsies, MRI of the dorsal root ganglion (DRG), and patient-reported outcomes.
Results: Of 11,221 patients with hernia surgery in 2018 identified, 8.5% had pain before that was relieved by surgery, but a similar percentage had novel pain in this region. Deep phenotyping of 141 healthy controls provided a map of the inguinal sensory system. The following analysis of patients with CPIP revealed that they suffered from moderate pain with neuropathic features, individual sensory abnormalities, and unilateral L1 DRG atrophy. In the blood, levels of C-C-motif chemokine ligand (CCL2) and brain-derived neurotrophic factor (BDNF) were upregulated, whereas apolipoprotein A1 (ApoA1) concentration was reduced. A cluster of DRG atrophy, BDNF, ApoA1, and anxiety correlated best with the diagnosis. CPIP patients with novel pain had significantly more DRG atrophy (-24% ipsilateral vs contralateral volume).
Conclusions: CPIP is often newly acquired after surgery. A combination of DRG imaging, serum markers, and anxiety screening can support the diagnosis. In the future, this could guide clinicians towards more personalised therapies (e.g. targeting anxiety or lipid profiles) and possible altered surgical techniques.
Clinical trial registration: German Trial Registry DRKS00024588 and DRKS00016790.
Keywords: chronic postsurgical pain; cytokines; dorsal root ganglion; hernia surgery; imaging; lipids.
Copyright © 2025 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declarations of interests HR received consultant fees from Gruenenthal and Orion, and financial support for a study by Algiax. WM reports grants from Gruenenthal and Pfizer, personal fees from Tafalgie, Kyowa, Mundipharma, Grünenthal, Ethypharm, and Spectrum Therapeutics. CS has received consulting fees from Algiax, Bayer, Grifols, Immunic, Merz, Roche, and Takeda Pharmaceuticals, and has given educational talks for Teva, CSL Behring, Grifols, GlaxoSmithKline, Takeda Pharmaceuticals, Pfizer, Amicus, and Alnylam. All other authors have no conflict of interest regarding this work.
Figures




References
-
- Poobalan A.S., Bruce J., Smith W.C., King P.M., Krukowski Z.H., Chambers W.A. A review of chronic pain after inguinal herniorrhaphy. Clin J Pain. 2003;19:48–54. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
