

Differential protection against SARS-CoV-2 reinfection pre- and post-Omicron
- PMID: 39910292
- PMCID: PMC11946897
- DOI: 10.1038/s41586-024-08511-9
Differential protection against SARS-CoV-2 reinfection pre- and post-Omicron
Abstract
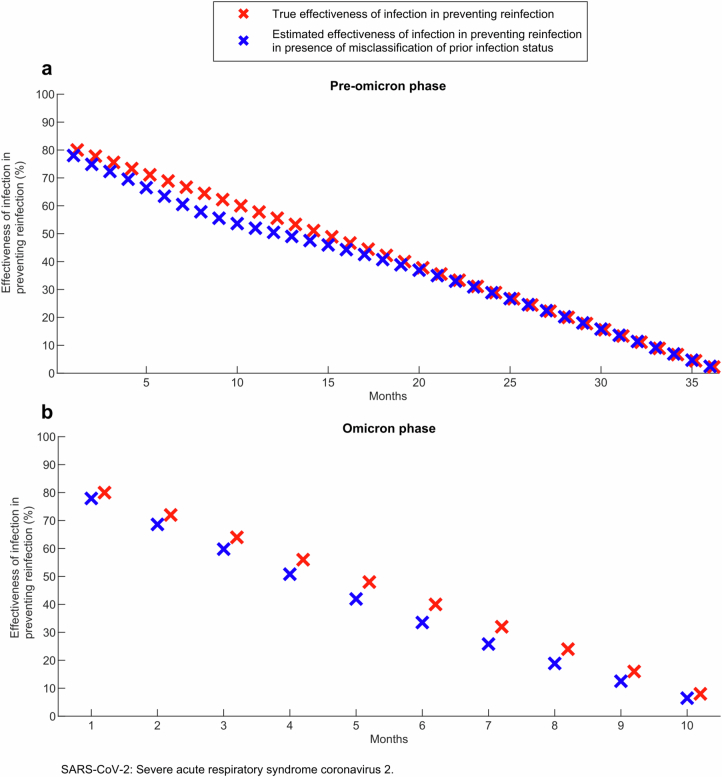
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly evolved over short timescales, leading to the emergence of more transmissible variants such as Alpha and Delta1-3. The arrival of the Omicron variant marked a major shift, introducing numerous extra mutations in the spike gene compared with earlier variants1,2. These evolutionary changes have raised concerns regarding their potential impact on immune evasion, disease severity and the effectiveness of vaccines and treatments1,3. In this epidemiological study, we identified two distinct patterns in the protective effect of natural infection against reinfection in the Omicron versus pre-Omicron eras. Before Omicron, natural infection provided strong and durable protection against reinfection, with minimal waning over time. However, during the Omicron era, protection was robust only for those recently infected, declining rapidly over time and diminishing within a year. These results demonstrate that SARS-CoV-2 immune protection is shaped by a dynamic interaction between host immunity and viral evolution, leading to contrasting reinfection patterns before and after Omicron's first wave. This shift in patterns suggests a change in evolutionary pressures, with intrinsic transmissibility driving adaptation pre-Omicron and immune escape becoming dominant post-Omicron, underscoring the need for periodic vaccine updates to sustain immunity.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.A.B. has received institutional grant funding from Gilead Sciences unrelated to the work presented in this paper. The other authors declare no competing interests.
Figures









References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
