

Indications, contributing factors, and short-term outcomes of pneumonectomy: an 8-year retrospective study in a resource-limited setting
- PMID: 39910675
- PMCID: PMC11796055
- DOI: 10.1186/s13019-024-03268-8
Indications, contributing factors, and short-term outcomes of pneumonectomy: an 8-year retrospective study in a resource-limited setting
Abstract
Background: Pneumonectomy, the surgical removal of an entire lung, was first performed in 1933 by Evarts A. Graham for lung carcinoma. Today, pneumonectomy is primarily indicated for non-small cell lung cancer (NSCLC) worldwide. However, it carries a higher risk of morbidity and mortality compared to less extensive lung resections.
Objectives: This study aims to investigate the indications for pneumonectomy and its short-term outcomes among patients who underwent the procedure between 2016 and 2023.
Methods and materials: A retrospective study was conducted on 112 patients who underwent pneumonectomy. Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25. Univariate, bivariate, and multivariate analyses were performed to address the study's objectives. The Pearson chi-square test, crude odds ratio (COR), and adjusted odds ratio (AOR) were calculated for categorical variables where appropriate. To identify factors associated with pneumonectomy, a binary logistic regression model was used, and odds ratios with 95% confidence intervals were calculated. A p-value of < 0.25 was used as a threshold for including variables in the multivariate analysis, while a p-value of < 0.05 was considered statistically significant in the final model.
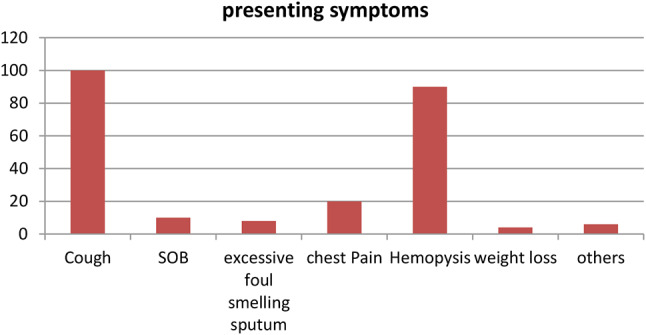
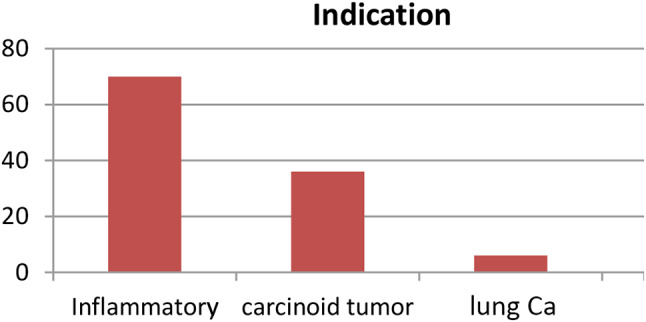
Results: The majority of patients were aged between 20 and 30 years, with 54 patients (48.2%) in this age group, and a male-to-female ratio of 1.6:1. The primary indication for pneumonectomy was inflammatory conditions, accounting for 62.5% (70 patients), followed by carcinoid tumors at 32.1% (36 patients). Lung cancer was the diagnosis in 5.4% (6 patients) of cases. Factors significantly associated with pneumonectomy included a history of tuberculosis treatment (AOR 40.3; 95% CI: 3.01, 540.2), intraoperative blood loss > 500 mL (AOR 9.07; 95% CI: 1.04, 79.13), and surgical duration > 180 min (AOR 37.9; 95% CI: 1.82, 792.3). The morbidity rate was 25%, while the mortality rate was 5.4%.
Conclusion and recommendations: In our setting, pneumonectomy is most commonly performed for inflammatory conditions. Significant factors associated with the procedure include a history of tuberculosis treatment, intraoperative blood loss > 500 mL, and surgical duration > 180 min. To reduce the need for pneumonectomy, strategies should focus on tuberculosis prevention, screening, and proper patient evaluation and diagnosis before treatment, to prevent extensive lung damage that often necessitates this procedure.
Keywords: Benign lung disease; Morbidity; Mortality; Pneumonectomy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical considerations and consent to participate: Ethical approval for the study was obtained from the Research Ethics Committee of the Department of Surgery/Institutional Review Board (IRB) of Addis Ababa University College of Health Sciences (AAU CHS) before data collection began. Medical record numbers were used for data collection, and personal identifiers of patients were not included in the research report to maintain anonymity. Access to the collected data was restricted to the principal investigator, ensuring that confidentiality was upheld throughout the project. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Beshara M, Bora V. Pneumonectomy. [Updated 2022 Sep 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555969/
-
- Al-Ghuzey A, Daffar AA, Al-Temimi RRH, et al. A retrospective study of pneumonectomy: review of 100 cases in Al-Hussein teaching hospital/Thi-Qar (2013–2020). Curr Pediatr Res. 2022;26(5):1427–32.
-
- Brunelli A, Kim AW, Berger KI, et al. Physiologic evaluation of the patient with lung cancer being considered for sectional surgery: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:166–90. [Crossref][Google Scholar][Pubmed]. - PubMed
-
- Blyth DF. Pneumonectomy for inflammatory lung disease. Eur J Cardiothorac Surg. 2000;18(4):429 – 34. 10.1016/s1010-7940(00)00526-1. PMID: 11024380. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
