

Haemodiafiltration versus high-flux haemodialysis-a Consensus Statement from the EuDial Working Group of the ERA
- PMID: 39914451
- PMCID: PMC12378613
- DOI: 10.1093/ndt/gfaf024
Haemodiafiltration versus high-flux haemodialysis-a Consensus Statement from the EuDial Working Group of the ERA
Abstract
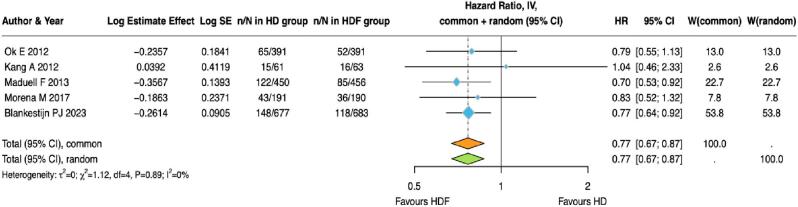
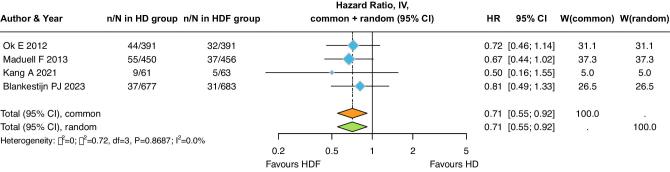
Haemodialysis (HD) is a life-saving therapy for individuals with kidney failure. Post-filter haemodiafiltration (HDF) and high-flux HD are the most widely used treatment modalities. To date, five randomized controlled trials (RCTs) have been performed that compare all-cause and cardiovascular (CV) mortality between HDF and low- or high-flux HD in adults receiving maintenance dialysis for at least 1 year. RCTs, meta-analyses and pooled individual patient data analyses have been published on this topic. However, all of them are limited by the heterogeneity of inclusion criteria and significant methodological shortcomings, including informative selection bias and the exclusion of poorly performing patients from the HDF arm after randomization. Given this background, the European Dialysis Working Group of the European Renal Association presents a Consensus Statement on HDF and high-flux HD, addressing three key outcomes: survival, health-related quality of life, and biochemical endpoints. A separate section is dedicated to paediatric patients. We searched five large electronic databases to identify parallel or cross-over RCTs comparing HDF with high-flux HD on pre-defined outcome measures. Using a mini-Delphi method, we developed 22 key consensus points by combining meta-analyses, clinical experience, and expert opinion. They aim to inform and assist in decision making and are not intended to define a standard of care. The key summary point is that HDF appears to be associated with improved overall and CV survival, provided high convection volumes are achieved. The generalizability of these findings to the entire dialysis population depends on the patient's overall health and requires further study.
Keywords: all-cause mortality; convection volume; haemodiafiltration; haemodialysis; kidney failure.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
R.S. discloses research grants from Fresenius Medical Care and Vitaflo, consulting fees from Astra Zeneca, and speaker honoraria from Fresenius Medical Care and Amgen; B.M. is a senior clinical investigator of the Fonds Wetenschappelijk Onderzoek (grant 1800820 N) and received support from KU Leuven via grants 3M190551 and C14/21/103. He received speaker and/or consultancy fees from Baxter, Nipro, Fresenius; I.N. discloses speaker honoraria from Fresenius KABI and Astra Zeneca; A.D. received a travel grant from Nipro Corporation, Japan, and speaker honoraria from Fresenius Medical Care; Y.B. discloses speaker honoraria from Astra Zeneca; C.C. received consultancy fees from Rhythm and Maze Therapeutics, and travel support from Amgen and Sanofi; and the other authors declare no conflict of interest.
Figures










References
-
- Cheung AK, Leypoldt JK.. The hemodialysis membranes: a historical perspective, current state and future prospect. Semin Nephrol 1997;17:196–213. - PubMed
-
- Henderson LW, Colton CK, Ford CA.. Kinetics of hemodiafiltration: II. Clinical characterization of a new blood cleansing modality. J Lab Clin Med 1975;85:372–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
