

Swarm learning with weak supervision enables automatic breast cancer detection in magnetic resonance imaging
- PMID: 39915630
- PMCID: PMC11802753
- DOI: 10.1038/s43856-024-00722-5
Swarm learning with weak supervision enables automatic breast cancer detection in magnetic resonance imaging
Abstract
Background: Over the next 5 years, new breast cancer screening guidelines recommending magnetic resonance imaging (MRI) for certain patients will significantly increase the volume of imaging data to be analyzed. While this increase poses challenges for radiologists, artificial intelligence (AI) offers potential solutions to manage this workload. However, the development of AI models is often hindered by manual annotation requirements and strict data-sharing regulations between institutions.
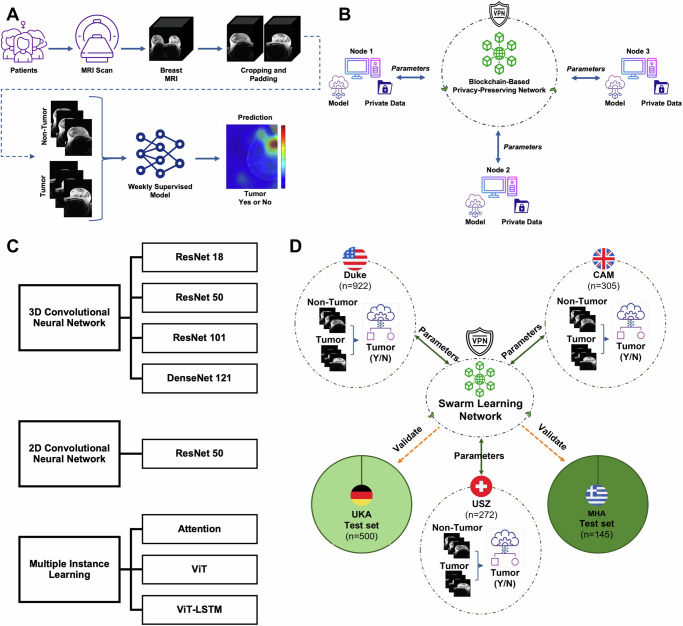
Methods: In this study, we present an integrated pipeline combining weakly supervised learning-reducing the need for detailed annotations-with local AI model training via swarm learning (SL), which circumvents centralized data sharing. We utilized three datasets comprising 1372 female bilateral breast MRI exams from institutions in three countries: the United States (US), Switzerland, and the United Kingdom (UK) to train models. These models were then validated on two external datasets consisting of 649 bilateral breast MRI exams from Germany and Greece.
Results: Upon systematically benchmarking various weakly supervised two-dimensional (2D) and three-dimensional (3D) deep learning (DL) methods, we find that the 3D-ResNet-101 demonstrates superior performance. By implementing a real-world SL setup across three international centers, we observe that these collaboratively trained models outperform those trained locally. Even with a smaller dataset, we demonstrate the practical feasibility of deploying SL internationally with on-site data processing, addressing challenges such as data privacy and annotation variability.
Conclusions: Combining weakly supervised learning with SL enhances inter-institutional collaboration, improving the utility of distributed datasets for medical AI training without requiring detailed annotations or centralized data sharing.
Plain language summary
Breast cancer screening guidelines are expanding to include more MRI scans, increasing the amount of imaging data doctors must analyze. This study explored how artificial intelligence (AI) can help manage this increased workload while overcoming challenges such as limited data sharing between hospitals and the need for detailed annotations on each image. Researchers used MRI scans from five hospitals in the US, Switzerland, the UK, Germany, and Greece to train and test AI models. They found that a specific type of AI model performed the best, and that training AI collaboratively across hospitals improved results compared to training at individual sites. This approach could make AI tools more effective and secure for use in healthcare, potentially improving breast cancer detection and patient outcomes.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: J.N.K. declares consulting services for Owkin, France, and Panakeia, UK, and has received honoraria for lectures by Bayer, Eisai, MSD, BMS, Roche, Pfizer, and Fresenius. J.N.K. and D.T. hold shares in StratifAI GmbH, Germany. S.M. declares employment and shareholding with Osimis, Belgium. No other potential conflicts of interest are declared by any of the authors. The authors received advice from the customer support team of Hewlett Packard Enterprise (HPE) when performing this study, but HPE did not have any role in study design, conducting the experiments, interpretation of the results, or decision to submit for publication.
Figures


References
-
- Weinstein, S. P. et al. ACR appropriateness criteria® supplemental breast cancer screening based on breast density. J. Am. Coll. Radiol.18, S456–S473 (2021). - PubMed
LinkOut - more resources
Full Text Sources
