

Improved understanding of the respiratory drive pathophysiology could lead to earlier spontaneous breathing in severe acute respiratory distress syndrome
- PMID: 39916810
- PMCID: PMC11783659
- DOI: 10.1097/EA9.0000000000000030
Improved understanding of the respiratory drive pathophysiology could lead to earlier spontaneous breathing in severe acute respiratory distress syndrome
Abstract
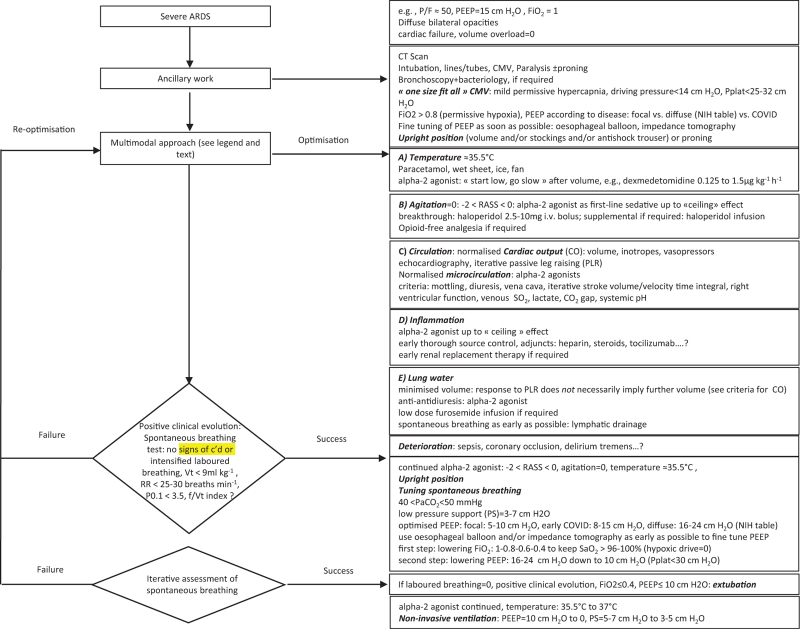
Optimisation of the respiratory drive, as early as possible in the setting of severe acute respiratory distress syndrome (ARDS) and not its suppression, could be a new paradigm in the management of severe forms of ARDS. Severe ARDS is characterised by tachypnoea and hyperpnoea, a consequence of a high respiratory drive. Some patients require endotracheal intubation, controlled mechanical ventilation (CMV) and paralysis to prevent overt ventilatory failure and self-inflicted lung injury. Nevertheless, intubation, CMV and paralysis do not address per se the high respiratory drive, they only suppress it. Optimisation of the respiratory drive could be obtained by a multimodal approach that targets attenuation of fever, agitation, systemic and peripheral acidosis, inflammation, extravascular lung water and changes in carbon dioxide levels. The paradigm we present, based on pathophysiological considerations, is that as soon as these factors have been controlled, spontaneous breathing could resume because hypoxaemia is the least important input to the respiratory drive. Hypoxaemia could be handled by combining positive end-expiratory pressure (PEEP) to prevent early expiratory closure and low pressure support to minimise the work of breathing (WOB). 'Cooperative' sedation with alpha-2 agonists, supplemented with neuroleptics if required, is the pharmacological adjunct, administered immediately after intubation as the first-line sedation regimen during the multimodal approach. Given relative contraindications (hypovolaemia, auriculoventricular block, sick sinus syndrome), alpha-2 agonists can help attenuate or moderate fever, increased oxygen consumption VO2, agitation, high cardiac output, inflammation and acidosis. They may also help to preserve microcirculation, cognition and respiratory rhythm generation, thus promoting spontaneous breathing. Returning the physiology of respiratory, ventilatory, circulatory and autonomic systems to normal will support the paradigm of optimised respiratory drive favouring early spontaneous ventilation, at variance with deep sedation, extended paralysis, CMV and use of the prone position as therapeutic strategies in severe ARDS.
Glossary: Glossary and Abbreviations_SDC.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Society of Anaesthesiology and Intensive Care.
Conflict of interest statement
Conflicts of interest: LQ reports honoraria and unrestricted research grants from Boehringer-Ingelheim, France, UCB Pharma, Belgium and Abbott International, Il, USA [1986-96] and holds US Patent 8 703 697: Method for treating early severe diffuse acute respiratory distress syndrome. J-MC reports personal fees and nonfinancial support from Drager, GE Healthcare, Sedana Medical, Baxter, and Amomed, personal fees from Fisher and Paykel Healthcare, Orion, Philips Medical, and Fresenius Medical Care, and nonfinancial support from LFB, and Bird Corporation, outside of the submitted work. DL reports honoraria from LFB, Edwards Lifesciences, Medtronic, Masimo, MSD and Aspen outside of the submitted work. The other authors disclose no conflict of interest.
Figures
Similar articles
-
Building on the Shoulders of Giants: Is the use of Early Spontaneous Ventilation in the Setting of Severe Diffuse Acute Respiratory Distress Syndrome Actually Heretical?Turk J Anaesthesiol Reanim. 2018 Sep;46(5):339-347. doi: 10.5152/TJAR.2018.01947. Epub 2018 Sep 1. Turk J Anaesthesiol Reanim. 2018. PMID: 30263856 Free PMC article. Review.
-
Combining O2 High Flow Nasal or Non-Invasive Ventilation with Cooperative Sedation to Avoid Intubation in Early Diffuse Severe Respiratory Distress Syndrome, Especially in Immunocompromised or COVID Patients?J Crit Care Med (Targu Mures). 2024 Oct 31;10(4):291-315. doi: 10.2478/jccm-2024-0035. eCollection 2024 Oct. J Crit Care Med (Targu Mures). 2024. PMID: 39916864 Free PMC article. Review.
-
Is there a place for pressure-support ventilation and high positive end-expiratory pressure combined to alpha-2 agonists early in severe diffuse acute respiratory distress syndrome?Med Hypotheses. 2013 Jun;80(6):732-7. doi: 10.1016/j.mehy.2013.02.023. Epub 2013 Apr 3. Med Hypotheses. 2013. PMID: 23561575
-
Early severe acute respiratory distress syndrome: What's going on? Part I: pathophysiology.Anaesthesiol Intensive Ther. 2016;48(5):314-338. doi: 10.5603/AIT.2016.0056. Anaesthesiol Intensive Ther. 2016. PMID: 28000204 Review.
-
Hypothesis: Fever control, a niche for alpha-2 agonists in the setting of septic shock and severe acute respiratory distress syndrome?Temperature (Austin). 2018 May 22;5(3):224-256. doi: 10.1080/23328940.2018.1453771. eCollection 2018. Temperature (Austin). 2018. PMID: 30393754 Free PMC article. Review.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, et al. . Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012; 307:2526–2533. - PubMed
-
- Guerin C, Thompson T, Brower R. The ten diseases that look like ARDS. Intensive Care Med 2015; 41:1099–1102. - PubMed
-
- Petitjeans F, Leroy S, Pichot C, et al. . Does interrupting self-induced lung injury and respiratory drive expedite early spontaneous breathing in the setting of early severe diffuse acute respiratory distress syndrome? Crit Care Med 2022; 50:1272–1276. - PubMed
-
- Telias I, Brochard L, Goligher EC. Is my patient's respiratory drive (too) high? Intensive Care Med 2018; 44:1936–1939. - PubMed
-
- Vaporidi K, Akoumianaki E, Telias I, et al. . Respiratory drive in critically ill patients. pathophysiology and clinical implications. Am J Respir Crit Care Med 2020; 201:20–32. - PubMed
LinkOut - more resources
Full Text Sources