

Socio-economic inequalities in access to COVID-19 tests in France in 2020: evidence from the EPICOV socio-epidemiological cohort
- PMID: 39917516
- PMCID: PMC11801222
- DOI: 10.3389/fpubh.2024.1434370
Socio-economic inequalities in access to COVID-19 tests in France in 2020: evidence from the EPICOV socio-epidemiological cohort
Abstract
Background: Testing for COVID-19 has been strongly recommended for individuals experiencing COVID-19-like symptoms or those with a close relative who tested positive. In France, tests were free of charge until mid-October 2021 and became widely available after June 2020. Our main objective was to investigate whether access to COVID-19 testing in France was associated with socio-economic conditions, considering gender and ethno-racial status.
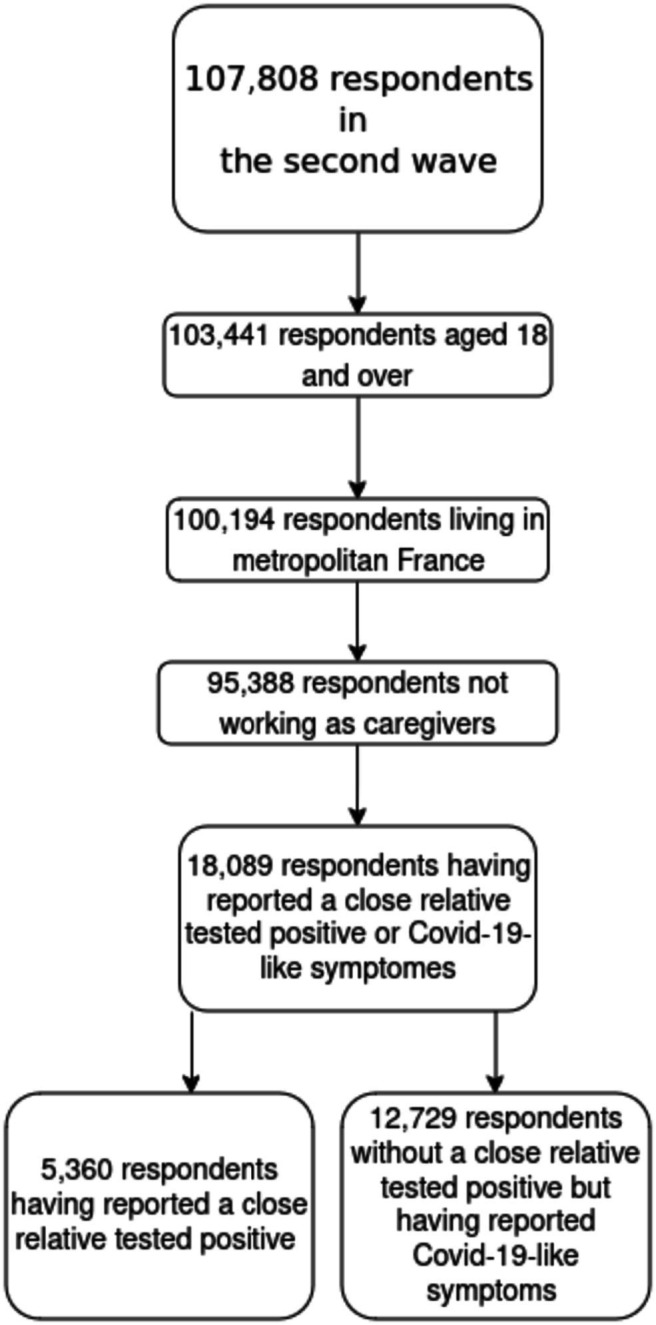
Methods: A random population-based cohort survey was conducted in France in May 2020 and November 2020, including 95,388 participants aged 18 and over. We used logistic regressions to identify how having been tested in 2020 was associated with socio-economic status and exposure factors among two groups of individuals. The first group consisted of individuals who had no close relative test positive but reported experiencing COVID-19-like symptoms, such as cough, fever, dyspnea, or sudden onset of ageusia, dysgeusia, or anosmia (N = 12,729). The second group included individuals, with or without symptoms, who reported that a close relative had tested positive for COVID-19 (N = 5,360).
Findings: In both groups, testing was more frequent among individuals living in urban areas. For individuals who had no close relative test positive but reported COVID-19-like symptoms, women were 1.04 (95%CI [1.01–1.06]) more likely than men to be tested, and testing decreased with age up to 35. Individuals holding a university degree were (1.08 [1.04–1.12]) more likely than those who only completed high school to be tested, as well as those in one of the three top income deciles with reference to the bottom decile (OR 1.07, [1.02–1.13] for the top decile). Ethno-racial status was not significantly associated with testing. For respondents who had a close relative test positive, testing was strongly associated with having experienced some symptoms, especially after September 1 (OR 1.34, 95%CI [1.30–1.39]). However, there was no link between testing and income, education, or ethno-racial status.
Interpretation: When an individual experiences symptoms but has no close relative who is positive, the motivation to test to avoid transmitting the virus to relatives by isolating oneself is particularly strong. This strategy makes sense when there are actual possibilities to isolate, which may explain why higher income and education positively impact the propensity to test. For individuals who had a close relative test positive, most socio-economic variables were no longer related to testing once infection risk was controlled for. The availability of tests at no cost is not sufficient in itself to eliminate socio-economic inequalities in testing.
Keywords: COVID-19; France; random survey; socio-economic inequalities; testing.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Similar articles
-
Social inequalities in medical appointment cancellations and reschedulings at the onset of the COVID-19 epidemic in France.Eur J Public Health. 2024 Aug 1;34(4):652-659. doi: 10.1093/eurpub/ckae101. Eur J Public Health. 2024. PMID: 38937956 Free PMC article.
-
Inequalities in access to prenatal care during the COVID-19 pandemic: Analysis of a population-based cohort.Paediatr Perinat Epidemiol. 2024 May;38(4):291-301. doi: 10.1111/ppe.13050. Epub 2024 Feb 10. Paediatr Perinat Epidemiol. 2024. PMID: 38339962
-
SARS-CoV-2 testing in North Carolina: Racial, ethnic, and geographic disparities.Health Place. 2021 May;69:102576. doi: 10.1016/j.healthplace.2021.102576. Epub 2021 Apr 19. Health Place. 2021. PMID: 33915376 Free PMC article.
-
The effect of social deprivation on the dynamic of SARS-CoV-2 infection in France: a population-based analysis.Lancet Public Health. 2022 Mar;7(3):e240-e249. doi: 10.1016/S2468-2667(22)00007-X. Epub 2022 Feb 15. Lancet Public Health. 2022. PMID: 35176246 Free PMC article.
-
Disparities in the distribution of COVID-19 testing sites in black and Latino areas in new York City.Prev Med. 2021 Jun;147:106463. doi: 10.1016/j.ypmed.2021.106463. Epub 2021 Feb 26. Prev Med. 2021. PMID: 33647352 Free PMC article.
References
-
- World Health Organization . Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases. Interim guidance. (2020). Available at: https://iris.who.int/bitstream/handle/10665/331329/WHO-COVID-19-laborato... (Accessed December 27, 2024).
-
- Green MA, García-Fiñana M, Barr B, Burnside G, Cheyne CP, Hughes D, et al. . Evaluating social and spatial inequalities of large scale rapid lateral flow SARS-CoV2 antigen testing in COVID-19 management: an observational study of Liverpool, UK (November 2020 to January 2021). Lancet Reg Health Europe. (2021) 6:100107. doi: 10.1016/j.lanepe.2021.100107, PMID: - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical