

Comprehensive characterization of micropapillary colorectal adenocarcinoma
- PMID: 39917902
- PMCID: PMC11880967
- DOI: 10.1002/path.6392
Comprehensive characterization of micropapillary colorectal adenocarcinoma
Abstract
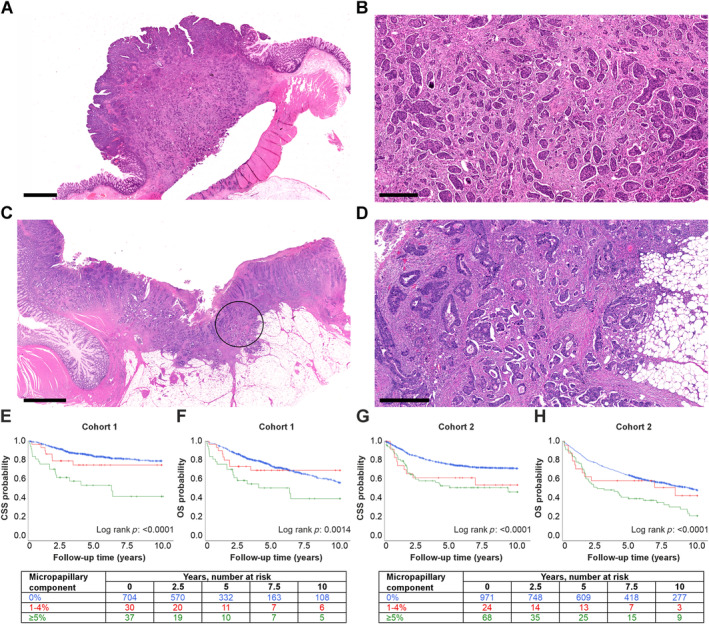
Micropapillary colorectal adenocarcinoma is a morphologic subtype of colorectal cancer (CRC) with insufficiently characterized prognostic significance and biological features. We analyzed the histopathological, immunological, and prognostic features of micropapillary adenocarcinoma in two independent CRC cohorts (N = 1,876). We found that micropapillary adenocarcinomas accounted for 4.9% and 6.4% of CRCs in the two cohorts. A micropapillary growth pattern was associated with advanced stage and lymphovascular invasion (p < 0.001), but also with shorter overall survival independent of these factors and other prognostic parameters (Cohort 1: hazard ratio [HR] 1.76, 95% confidence interval [CI] 1.08-2.87; Cohort 2: HR 1.47, 95% CI 1.08-2.00). Multiplex immunohistochemistry and machine learning-assisted image analysis showed that the micropapillary growth pattern was associated with decreased CD3+ T-cell and CD14+HLA-DR+ monocytic cell densities. Molecular features of micropapillary adenocarcinoma were studied using bioinformatic analyses in The Cancer Genome Atlas (TCGA) cohort (N = 629) and validated with optical genome mapping and immunohistochemistry. These analyses revealed that micropapillary adenocarcinomas frequently present with chromosome region 8q24 copy number gain, TP53 mutation, and overexpression of UPK2, MUC16, and epithelial-mesenchymal transition involved genes, such as L1CAM. These results indicate that micropapillary colorectal adenocarcinoma is an aggressive morphologic subtype of CRC characterized by shorter overall survival, decreased antitumorigenic immune response, and unique molecular features. Our findings support the classification of micropapillary adenocarcinoma as a distinct, high-risk subtype of CRC, which should be systematically evaluated in patient care. © 2025 The Author(s). The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
Keywords: bioinformatics; colorectal cancer; epithelial‐mesenchymal transition; immunology; micropapillary; multiplex immunohistochemistry; optical genome mapping; prognosis.
© 2025 The Author(s). The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
Figures



References
-
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024; 74: 229–263. - PubMed
-
- WHO Classification of Tumours Editorial Board . Digestive System Tumours (Vol. 1, 5th edn). International Agency for Research on Cancer: Lyon, 2019.
-
- Hugen N, Verhoeven RH, Lemmens VE, et al. Colorectal signet‐ring cell carcinoma: benefit from adjuvant chemotherapy but a poor prognostic factor. Int J Cancer 2015; 136: 333–339. - PubMed
-
- Keum NN, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol 2019; 16: 713–732. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
