

Challenges in the diagnosis of heart failure with preserved ejection fraction in individuals with obesity
- PMID: 39920805
- PMCID: PMC11806779
- DOI: 10.1186/s12933-025-02612-z
Challenges in the diagnosis of heart failure with preserved ejection fraction in individuals with obesity
Abstract
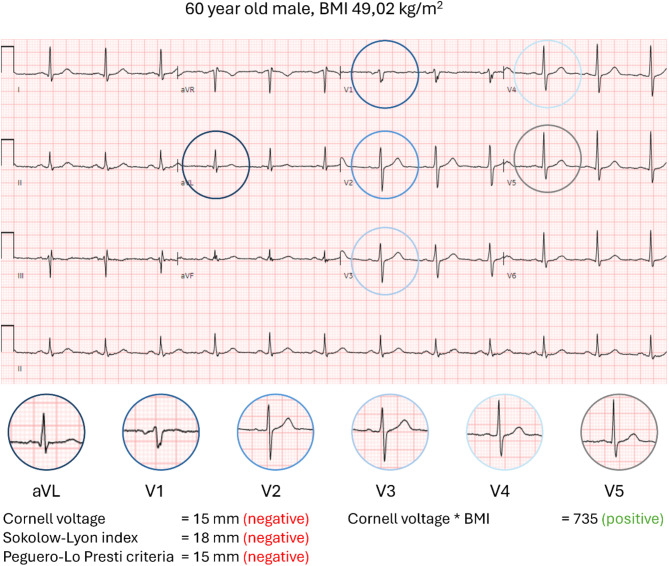
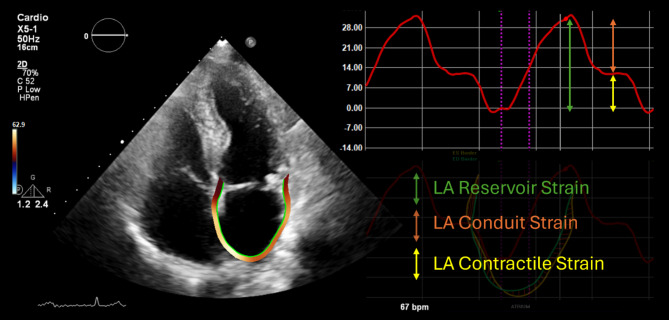
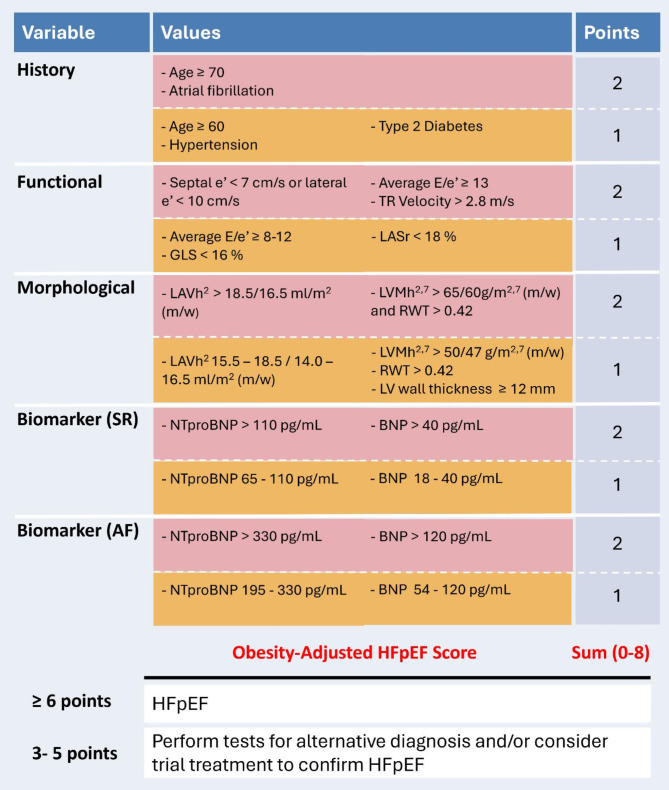
The rising prevalence of obesity and its association with heart failure with preserved ejection fraction (HFpEF) highlight an urgent need for a diagnostic approach tailored to this population. Diagnosing HFpEF is hampered by the lack of a single non-invasive diagnostic criterion. While this makes a firm diagnosis of HFpEF already notoriously difficult in the general population, it is even more challenging in individuals with obesity. The challenges stem from a range of factors, including the use of body mass index as a conceptually suboptimal indicator of health risks associated with increased body mass, symptom overlap between HFpEF and obesity, limitations in physical examination, difficulties in electrocardiographic and echocardiographic evaluation, and reduced diagnostic sensitivity of natriuretic peptides in individuals with obesity. In this review, we examine these diagnostic challenges and propose a diagnostic algorithm specifically tailored to improve the accuracy and reliability of HFpEF diagnosis in this growing patient demographic.
Keywords: Diagnosis; Echocardiography; Heart failure with preserved ejection fraction; Natriuretic peptides; Obesity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The institution of Dr. De Boer has received research grants and/or fees from Alnylam, AstraZeneca, Abbott, Bristol-Myers Squibb, Cardior Pharmaceuticals GmbH, NovoNordisk, and Roche; Dr. de Boer has had speaker engagements with and/or received fees from and/or served on an advisory board for Abbott, AstraZeneca, Bristol Myers Squibb, Cardior Pharmaceuticals GmbH, NovoNordisk, and Roche; Dr. de Boer received travel support from Abbott, Cardior Pharmaceuticals GmbH, and NovoNordisk. Dr Brugts reports speaker engagements and/or advisory to Astra Zeneca, Abbott, Bayer, Boehringer Ingelheim, Novartis and Vifor outside the submitted work (3 year period). The institution of Dr. Van Dalen received research grants from Biotronik SE & Co. KG, Boehringer Ingelheim, Pfizer, Daiichi Sankyo, Sanofi and Novo Nordisk.
Figures
References
-
- Obesity and overweight fact sheet World Health Organization. [Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
-
- Brouwers FP, de Boer RA, van der Harst P, Voors AA, Gansevoort RT, Bakker SJ, et al. Incidence and epidemiology of new onset heart failure with preserved vs. reduced ejection fraction in a community-based cohort: 11-year follow-up of PREVEND. Eur Heart J. 2013;34(19):1424–31. - PubMed
-
- Kitzman DW, Shah SJ. The HFpEF obesity phenotype: the elephant in the room. J Am Coll Cardiol. 2016;68(2):200–3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
