

Physiology and pathophysiology of mucus and mucolytic use in critically ill patients
- PMID: 39920835
- PMCID: PMC11806889
- DOI: 10.1186/s13054-025-05286-x
Physiology and pathophysiology of mucus and mucolytic use in critically ill patients
Abstract
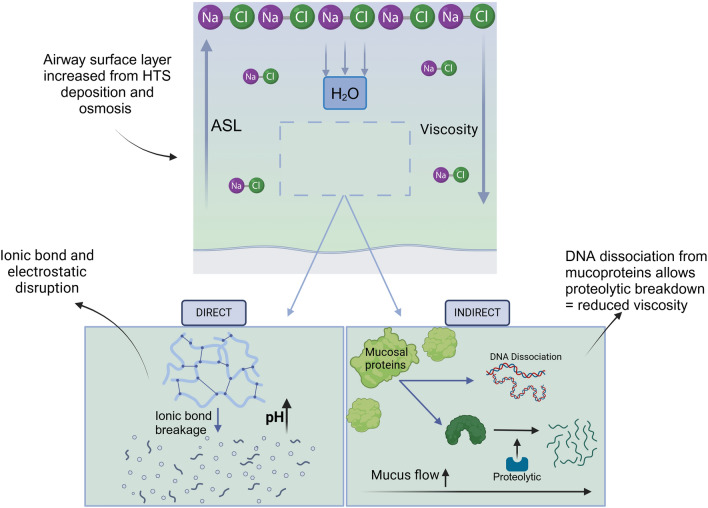
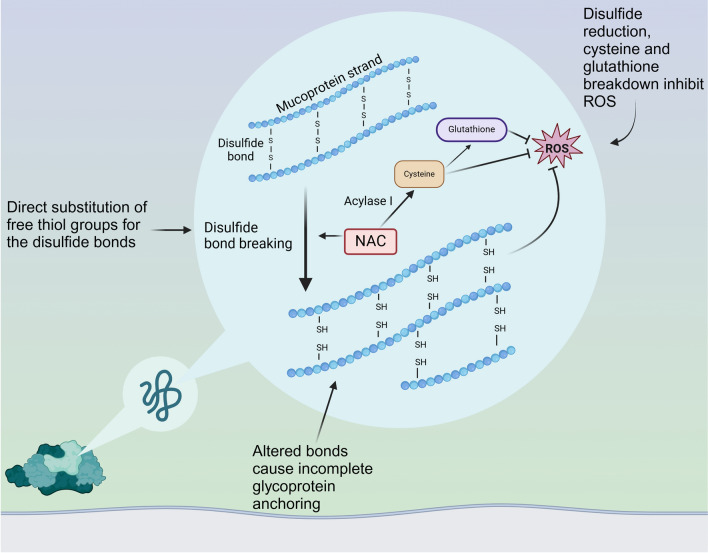
Airway mucus is a highly specialised secretory fluid which functions as a physical and immunological barrier to pathogens whilst lubricating the airways and humifying atmospheric air. Dysfunction is common during critical illness and is characterised by changes in production rate, chemical composition, physical properties, and inflammatory phenotype. Mucociliary clearance, which is determined in part by mucus characteristics and in part by ciliary function, is also dysfunctional in critical illness via disease related and iatrogenic mechanisms. The consequences of mucus dysfunction are potentially devastating, contributing to prolonged ventilator dependency, increased risk of secondary pneumonia, and worsened lung injury. Mucolytic therapies are designed to decrease viscosity, improve expectoration/suctioning, and thereby promote mucus removal. Mucolytics, including hypertonic saline, dornase alfa/rhDNase, nebulised heparin, carbocisteine/N-Acetyl cysteine, are commonly used in critically ill patients. This review summarises the physiology and pathophysiology of mucus and the existing evidence for the use of mucolytics in critically ill patients and speculates on journey to individualised mucolytic therapy.
Keywords: Critical care; Intensive care; Mechanical ventilation; Mucolytics.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable in this review. Consent for publication: Not applicable in this review. Competing interests: The authors declare no competing interests.
Figures





References
-
- Bansil R, Turner BS. The biology of mucus: Composition, synthesis and organization. Adv Drug Deliv Rev. 2018;124:3–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
