

Early COVID-19 and protection from Omicron in a highly vaccinated population in Ontario, Canada: a matched prospective cohort study
- PMID: 39923009
- PMCID: PMC11806543
- DOI: 10.1186/s12879-024-10331-1
Early COVID-19 and protection from Omicron in a highly vaccinated population in Ontario, Canada: a matched prospective cohort study
Abstract
Objectives: Predictions regarding the on-going burden of SARS-CoV-2, and vaccine recommendations, require an understanding of infection-associated immune protection. We assessed whether early COVID-19 provided protection against Omicron infection.
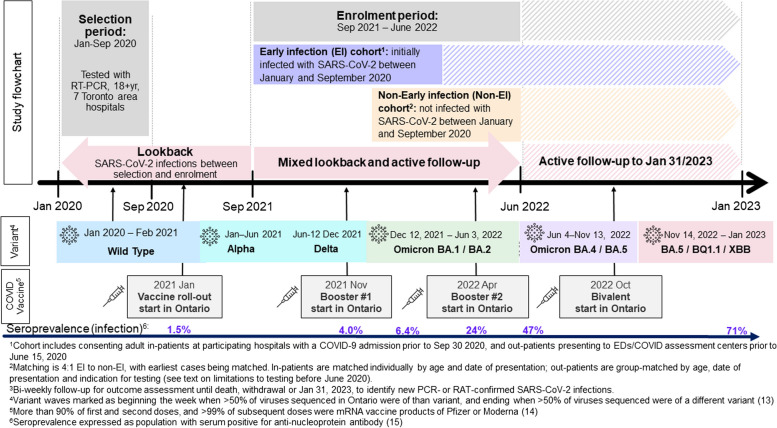
Methods: We enrolled a cohort of adults in Ontario, Canada, with COVID-19 prior to October 2020 (early infection, EI), and a matched cohort with COVID-19 testing and a negative PCR (non-EI). Participants completed baseline surveys then surveys every two weeks until January 2023. Multivariable Cox regression was used to assess factors associated with COVID-19 infection during the first 14 months of Omicron.
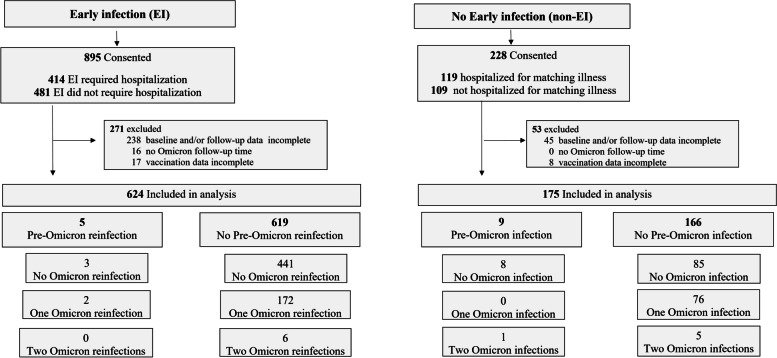
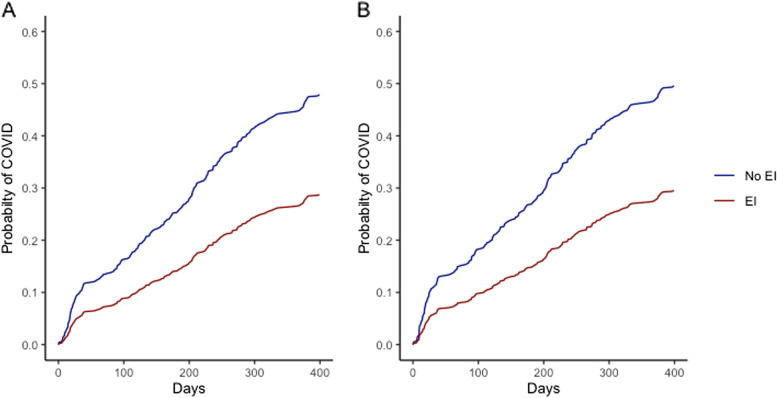
Results: Overall, 624 EI (70%) and 175 (77%) non-EI participants met criteria for analysis; 590 (95%) EI and 164 (94%) non-EI had received at least 2 COVID-19 vaccine doses prior to Omicron. Of 624 EI, 175 (28%) had one SARS-CoV-2 re-infection and 8 (1.3%) had two, compared to 84 (48%) non-EI participants with one, 5 (2.9%) with two and 1 (0.6%) with 3 infections (P < 0.0001). In multivariable analysis of risk factors for Omicron infection, the overall hazard ratio (HR, 95%CI) associated with EI was 0.56 (0.43-0.74); HRs for BA.1/2, BA.4/5 and mixed BA.5/BQ.1/XBB periods were 0.66 (0.45-0.97), 0.44 (0.28-0.68) and 0.71 (0.32-1.56). EI and BA.1/2 infection combined reduced later Omicron infection (HR 0.07 (0.03-0.21) compared to no prior infection. Older age, non-White ethnicity, no children in household, and lower neighbourhood income were associated with reduced risk of infection.
Conclusions: In our highly vaccinated population, early SARS-CoV-2 infection was associated with a 44% reduction in symptomatic COVID-19 during the first 14 months of Omicron, providing significant protection against re-infection for more than 2 years.
Keywords: COVID-19; Re-infection; SARS-CoV-2 infection; Vaccination.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Informed consent was obtained from all study participants. The study was approved by the research ethics boards of participating hospitals (North York General #2024-0233-1025; Sunnybrook Health Sciences Centre #149–1994; Michael Garron Hospital #084-0209-Lab-01, University Health Network #14-8339-AE, The Scarborough Health Network #MED-02-011, William Osler Health System #95 − 0001, and Mount Sinai Hospital #21-0069-E). Consent for publication: Not applicable. Competing interests: MHK, CM, MM, PZ, JV, JY and JMM are employees and shareholders of Pfizer Inc. AM declares grants and personal fees from Pfizer, grants from Sanofi, personal fees from AstraZeneca, GlaxoSmithKline, Moderna and Novavax, outside the submitted work. ACG has received research funds from Providence Therapeutics Holdings, Inc., outside the submitted work. All other authors, no conflicts of interest.
Figures
Similar articles
-
Protection Conferred by COVID-19 Vaccination, Prior SARS-CoV-2 Infection, or Hybrid Immunity Against Omicron-Associated Severe Outcomes Among Community-Dwelling Adults.Clin Infect Dis. 2024 May 15;78(5):1372-1382. doi: 10.1093/cid/ciad716. Clin Infect Dis. 2024. PMID: 38001037 Free PMC article.
-
BNT162b2 vaccine protection against omicron and effect of previous infection variant and vaccination sequence among children and adolescents in Singapore: a population-based cohort study.Lancet Child Adolesc Health. 2023 Jul;7(7):463-470. doi: 10.1016/S2352-4642(23)00101-3. Epub 2023 May 15. Lancet Child Adolesc Health. 2023. PMID: 37201540 Free PMC article.
-
Clinical profile analysis of SARS-CoV-2 community infections during periods with omicron BA.2, BA.4/5, and XBB dominance in Hong Kong: a prospective cohort study.Lancet Infect Dis. 2025 Mar;25(3):276-289. doi: 10.1016/S1473-3099(24)00574-7. Epub 2024 Oct 14. Lancet Infect Dis. 2025. PMID: 39419049
-
Past SARS-CoV-2 infection protection against re-infection: a systematic review and meta-analysis.Lancet. 2023 Mar 11;401(10379):833-842. doi: 10.1016/S0140-6736(22)02465-5. Epub 2023 Feb 16. Lancet. 2023. PMID: 36930674 Free PMC article.
-
Clinical Manifestations of SARS-CoV-2 Infection in Immunocompetent Adults in the Era of Widespread Population Immunity and Omicron Sublineage Viruses.Infect Dis Clin North Am. 2025 Jun;39(2):233-251. doi: 10.1016/j.idc.2025.02.002. Epub 2025 Mar 10. Infect Dis Clin North Am. 2025. PMID: 40068975 Review.
References
-
- Reiner RC, Collins JK, Murray CJL. Forecasting the trajectory of the COVID-19 pandemic into 2023 under plausible variant and intervention scenarios: a global modelling study. medRxiv, 10.1101/2023030723286952. 2023. - DOI
-
- World Health Organization. Coronavirus (COVID-19) Dashboard. https://covid19.who.int/. Accessed August 6, 2023.
-
- World Health Organization. Interim statement on hybrid immunity and increasing population seroprevalence rates. June 1. 2022. https://www.who.int/news/item/01-06-2022-interim-statement-on-hybrid-imm....
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
