

Clinical characterization of Collagen XII-related disease caused by biallelic COL12A1 variants
- PMID: 39923201
- PMCID: PMC11920742
- DOI: 10.1002/acn3.52225
Clinical characterization of Collagen XII-related disease caused by biallelic COL12A1 variants
Abstract
Objective: While there have been several reports of patients with dominantly acting COL12A1 variants, few cases of the more severe recessive Collagen XII-related disorders have previously been documented.
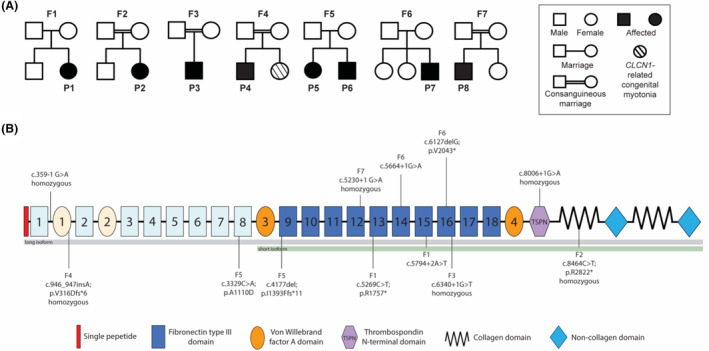
Methods: We present detailed clinical, immunocytochemical, and imaging data on eight additional patients from seven families with biallelic pathogenic variants in COL12A1.
Results: All patients presented with a consistent constellation of congenital onset clinical features: hypotonia, dysmorphic features, most notably gingival hypertrophy, prominent distal joint hyperlaxity, with co-occurring contractures of large joints, and variable muscle involvement, evident both clinically and on muscle imaging. Five patients presented with a severe congenital phenotype manifesting with profound weakness, significantly delayed or minimal attainment of motor milestones, respiratory insufficiency, and feeding difficulties. Three patients presented with mild-to-moderate muscle weakness and delayed milestones but were able to achieve independent ambulation. Patients were found to have biallelic loss-of-function COL12A1 variants, except for one family (p.I1393Ffs*11/p.A1110D). Consistent with the variable clinical spectrum, in vitro immunocytochemistry analysis in fibroblasts ranged from complete absence of Collagen XII expression in a patient with severe disease, to a mild reduction in a patient with milder disease.
Interpretation: Here we characterize the clinical presentation, muscle imaging, and dermal fibroblast immunostaining findings associated with biallelic variants in COL12A1, further establishing COL12A1 as a recessive myopathic Ehlers-Danlos syndrome (mEDS) gene, and expanding the clinical spectrum to include a milder EDS phenotype.
© 2024 The Author(s). Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures



References
-
- Veit G, Hansen U, Keene DR, et al. Collagen XII interacts with avian tenascin‐X through its NC3 domain. J Biol Chem. 2006;281(37):27461‐27470. - PubMed
-
- Chiquet M. Regulation of extracellular matrix gene expression by mechanical stress. Matrix Biol. 1999;18(5):417‐426. - PubMed
-
- Hicks D, Farsani GT, Laval S, et al. Mutations in the collagen XII gene define a new form of extracellular matrix‐related myopathy. Hum Mol Genet. 2014;23(9):2353‐2363. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
