

Effects of conditional cash transfers and pre-test and post-test tuberculosis counselling on patient outcomes and loss to follow-up across the continuum of care in South Africa: a randomised controlled trial
- PMID: 39923785
- PMCID: PMC12176662
- DOI: 10.1016/S1473-3099(24)00816-8
Effects of conditional cash transfers and pre-test and post-test tuberculosis counselling on patient outcomes and loss to follow-up across the continuum of care in South Africa: a randomised controlled trial
Abstract
Background: Economic and behavioural factors lead to poor outcomes in patients with tuberculosis. We investigated the effects of a package of interventions consisting of pre-test and post-test tuberculosis counselling with conditional cash transfers on patient outcomes in adults undergoing investigation for pulmonary tuberculosis.
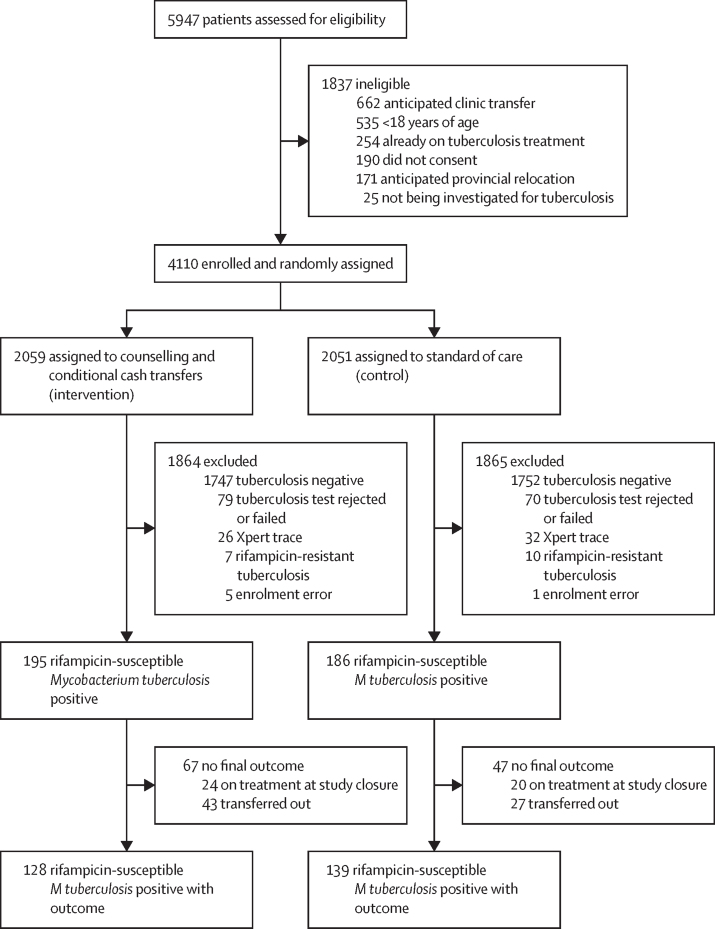
Methods: This pragmatic, open-label, individual randomised controlled trial was done in nine clinics in Johannesburg, South Africa. Participants (aged ≥18 years) undergoing investigation for tuberculosis were randomly assigned (1:1) to the intervention group or control group (standard of care) via permuted block randomisation, stratified by clinic; group assignment was concealed using opaque envelopes. The intervention group received pre-test and post-test tuberculosis counselling, and for participants diagnosed with rifampicin-susceptible tuberculosis, a digital payment (R150; approximately US$10) at treatment initiation and each monthly treatment visit. Payments were contingent on timely attendance: 14 days from initial sputum sample collection and within 7 days on either side of their scheduled monthly appointment. The primary endpoint was successful patient outcome (patients who were cured or completed treatment) or unsuccessful patient outcome (pretreatment loss-to-follow-up, on-treatment loss-to-follow-up, development of rifampicin-resistant tuberculosis while on treatment, treatment failure [ie, smear or culture positive at 5 months or later after commencing treatment], or death). The primary outcome was analysed in the modified intention-to-treat population, defined as all randomly assigned participants with rifampicin-susceptible tuberculosis confirmed before the commencement of tuberculosis treatment. Weighted outcome prevalence, relative risks (RRs), and risk differences were calculated using a multivariable Poisson model with robust standard errors. This trial is registered with the Pan African Clinical Trials Registry (PACTR202410708311054) and is completed.
Findings: Between Oct 25, 2018, and Dec 9, 2019, 4110 participants were enrolled and randomly assigned, 2059 to the intervention group and 2051 to the control group. 381 (9·3%) participants had microbiologically confirmed rifampicin-susceptible pulmonary tuberculosis (195 [9·5%] of 2059 in the intervention group vs 186 [9·1%] of 2051 in the control group; median age 37 years [IQR 30 to 45], 257 [67·5%] male, 124 [32·5%] female). At study closure, primary outcome data were available for 128 (65·6%) of 195 participants in the intervention group and 139 (74·7%) of 186 participants in the control group. 105 (82·0%) of 128 participants in the intervention group and 93 (66·9%) of 139 participants in the control group had a successful patient outcome; 23 (18·0%) of 128 participants in the intervention group and 46 (33·1%) of 139 participants in the control group had an unsuccessful patient outcome. The weighted regression analysis showed a substantial reduction in the risk of unsuccessful patient outcomes in the intervention group compared with the control group (weighted prevalence 15·9% vs 28·6%; RR in weighted population 0·52, 95% CI 0·33 to 0·82; risk difference in weighted population -14·1 percentage points, 95% CI -23·3 to -4·8). Pretreatment loss to follow-up was lower in the intervention group than in the control group (unweighted population: five [3·9%] of 128 participants vs 22 [15·8%] of 139 participants; risk difference in weighted population -9·6 percentage points, 95% CI -14·9 to -4·2).
Interpretation: The package of interventions consisting of pre-test and post-test tuberculosis counselling with conditional cash transfers significantly reduced the risk of unsuccessful tuberculosis patient outcomes, bringing one of the 90-90-90 targets within reach (ie, achieving 90% tuberculosis treatment success). Furthermore, reduction in pretreatment loss to follow-up is expected to reduce transmission and lower incidence of the disease over time.
Funding: South African Medical Research Council, UK Medical Research Council, and Newton Fund.
Crown Copyright © 2025 Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license.
Conflict of interest statement
Declaration of interests SAM reports grants to their institution from the Bill & Melinda Gates Foundation, GSK, Pfizer, and MinervaX; clinical trial funding to their institution from Merck, Providence, and Gritstone; honoraria for lectures from GSK; and participation on data safety monitoring boards for PATH, CAPRISA, and Bavarian Nordic. All other authors declare no competing interests.
Similar articles
-
Safety, bactericidal activity, and pharmacokinetics of the antituberculosis drug candidate BTZ-043 in South Africa (PanACEA-BTZ-043-02): an open-label, dose-expansion, randomised, controlled, phase 1b/2a trial.Lancet Microbe. 2025 Feb;6(2):100952. doi: 10.1016/j.lanmic.2024.07.015. Epub 2025 Jan 7. Lancet Microbe. 2025. PMID: 39793592 Clinical Trial.
-
Immunogenicity, safety, and efficacy of the vaccine H56:IC31 in reducing the rate of tuberculosis disease recurrence in HIV-negative adults successfully treated for drug-susceptible pulmonary tuberculosis: a double-blind, randomised, placebo-controlled, phase 2b trial.Lancet Infect Dis. 2025 Jul;25(7):751-763. doi: 10.1016/S1473-3099(24)00814-4. Epub 2025 Mar 5. Lancet Infect Dis. 2025. PMID: 40056922 Clinical Trial.
-
Simultaneous initiation of dolutegravir-based antiretroviral therapy and once-weekly rifapentine and isoniazid for tuberculosis prevention in antiretroviral-naive people with HIV: an open-label, non-randomised, phase 1/2 trial.Lancet HIV. 2025 Jun;12(6):e428-e439. doi: 10.1016/S2352-3018(25)00002-5. Epub 2025 May 8. Lancet HIV. 2025. PMID: 40349709 Clinical Trial.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Nutritional interventions for survivors of childhood cancer.Cochrane Database Syst Rev. 2016 Aug 22;2016(8):CD009678. doi: 10.1002/14651858.CD009678.pub2. Cochrane Database Syst Rev. 2016. PMID: 27545902 Free PMC article.
Cited by
-
Lessons from a systematic tracing process aimed to reduce initial loss to follow-up (ILTFU) among people diagnosed with tuberculosis (TB) in Cape Town, South Africa.PLoS One. 2025 May 30;20(5):e0323943. doi: 10.1371/journal.pone.0323943. eCollection 2025. PLoS One. 2025. PMID: 40445886 Free PMC article.
References
-
- WHO Global tuberculosis report. 2024. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/globa...
-
- Nanoo A, Izu A, Ismail NA, et al. Nationwide and regional incidence of microbiologically confirmed pulmonary tuberculosis in South Africa, 2004–12: a time series analysis. Lancet Infect Dis. 2015;15:1066–1076. - PubMed
-
- Botha E, Den Boon S, Verver S, et al. Initial default from tuberculosis treatment: how often does it happen and what are the reasons? Int J Tuberc Lung Dis. 2008;12:820–823. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
