

The Association Between Pre-morbid Frailty and Discontinuation of Treatment Within 24 Hours in Critically Ill Older Adults Triaged to a Tertiary Care Emergency Department: A Retrospective Cohort Study
- PMID: 39925573
- PMCID: PMC11807291
- DOI: 10.7759/cureus.77222
The Association Between Pre-morbid Frailty and Discontinuation of Treatment Within 24 Hours in Critically Ill Older Adults Triaged to a Tertiary Care Emergency Department: A Retrospective Cohort Study
Abstract
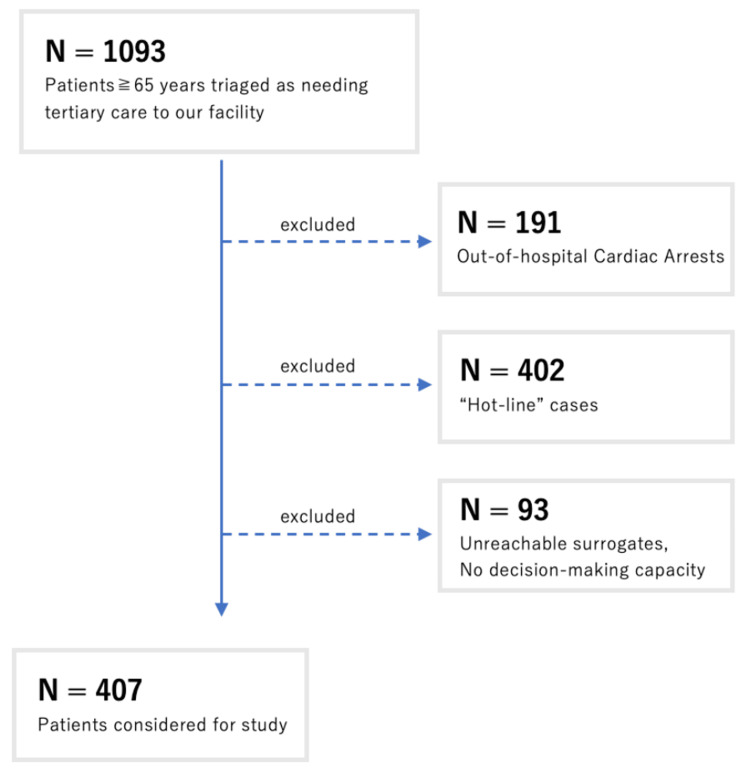
Background Some critically ill older adults would rather receive palliative than intensive care if their functional capacity and quality of life are compromised. Therefore, careful goals-of-care conversation is vital in frail older adults who are critically ill if there is no advance care planning before arrival at the emergency department. We considered that pre-morbid Clinical Frailty Scale (CFS) scores could be a potent factor in prioritizing such conversations if higher numbers were associated with increased withdrawal of treatment in these patients. This study aimed to investigate the association between pre-morbid frailty and discontinuation of treatment within 24 hours in older adults in Kobe, Japan. Methodology This retrospective, observational study was conducted among patients aged 65 and over who were triaged as needing tertiary care to our emergency department with subsequent admission for further treatment. The primary outcome was withdrawal of treatment within 24 hours. We examined the association between CFS and withdrawal of treatment using a multivariable logistic regression model with CFS 1-4 as a reference. Results During the study period, 1,093 patients were triaged to our emergency department as needing tertiary care. After exclusion, 407 patients (median age = 80 years (interquartile range = 73-87)), were included in the study. Of these, 58 (14.2%) patients withdrew from intensive care within 24 hours. The adjusted odds ratios were 1.99 for CFS 5 (95% confidence interval (CI) = 0.74-5.32, p = 0.17), 2.48 for CFS 6 (95% CI = 0.93-6.57, p = 0.068), and 5.48 for CFS 7-9 (95% CI = 2.68-12.6, p < 0.01). Conclusions Higher CFS scores in critically ill older adults were associated with a higher likelihood of withdrawal within 24 hours. The goals-of-care conversation could be held proactively when CFS scores are high to reduce unwanted medical intervention.
Keywords: advanced care planning; clinical frailty scale; goal of care; pre-hospital intervention; withdrawal of care.
Copyright © 2025, Tanaka et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
-
- Palliative care physicians' practices and attitudes regarding advance care planning in palliative care units in Japan: a nationwide survey. Nakazawa K, Kizawa Y, Maeno T, Takayashiki A, Abe Y, Hamano J, Maeno T. Am J Hosp Palliat Care. 2014;31:699–709. - PubMed
-
- Grisso T, Appelbaum PS. Assessing Competence to Consent to Treatment: A Guide for Physicians and Other Health Professionals. New York, NY: Oxford University Press; 1998. Abilities related to competence.
LinkOut - more resources
Full Text Sources