

68Ga-pentixafor PET/CT in guiding surgical management of primary aldosteronism
- PMID: 39926105
- PMCID: PMC11803161
- DOI: 10.1016/j.jcte.2025.100384
68Ga-pentixafor PET/CT in guiding surgical management of primary aldosteronism
Abstract
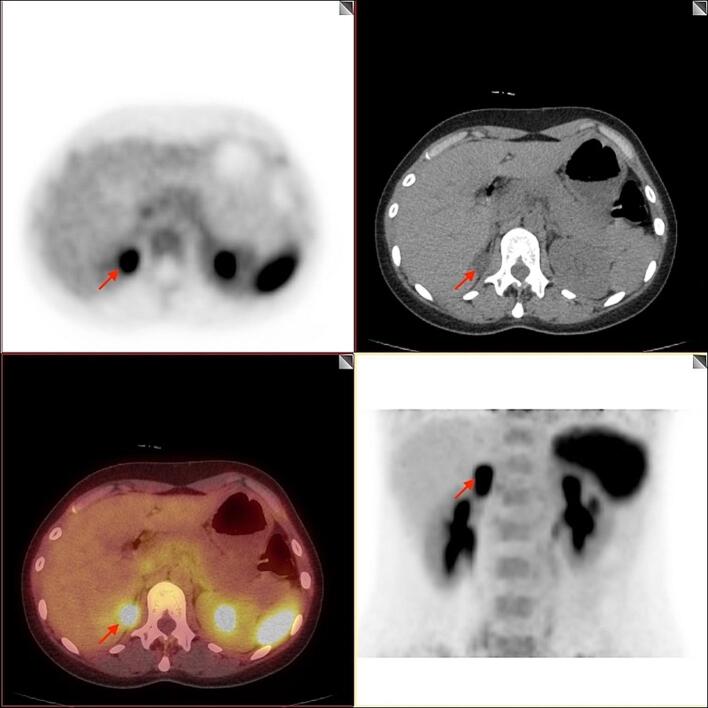
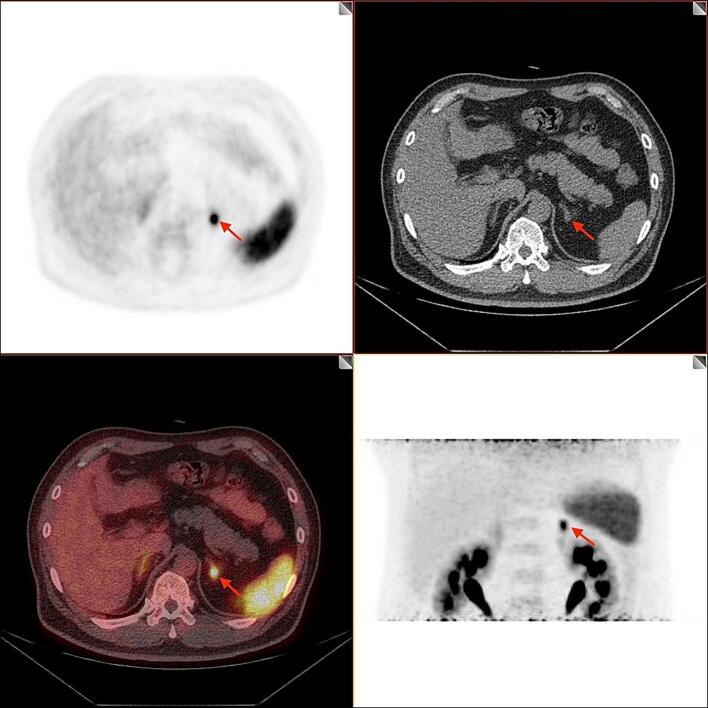
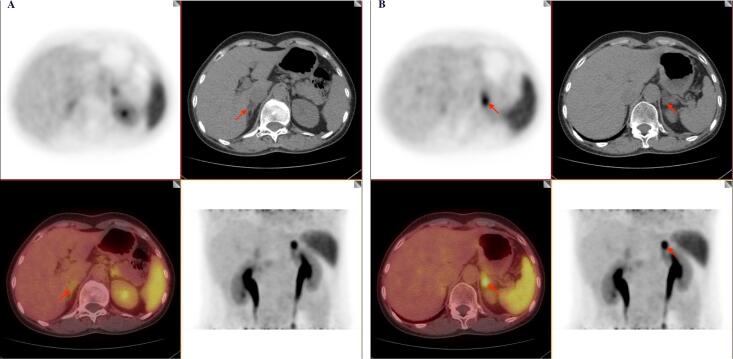
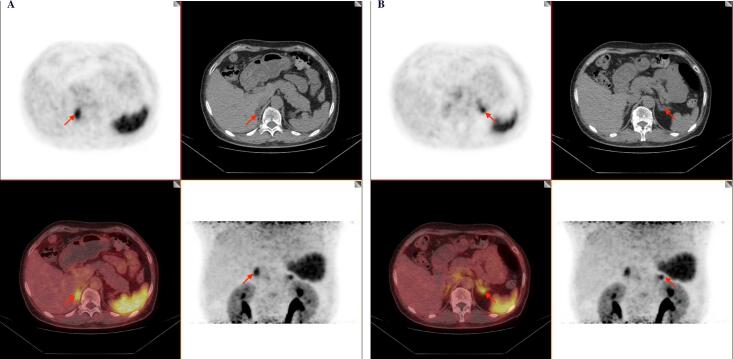
Purpose: This study aimed to explore the significance of 68Ga-pentixafor PET/CT in guiding surgical treatments for primary aldosteronism (PA) patients, by identifying functional lesions and determining the dominant side of aldosterone secretion.
Materials and methods: We prospectively included 91 PA patients receiving surgical treatments based on the results of 68Ga-pentixafor PET/CT. The 68Ga-pentixafor PET/CT images were evaluated by visual and semi-quantitative analysis. The relationship between radionuclide imaging characteristics and postoperative outcomes was assessed following surgery.
Results: The positive detection rate of 68Ga-pentixafor PET/CT in 91 PA patients was 85.7 % (78/91) with a median maximum standardized uptake value (SUVmax) of 10.2 (6.0-16.0). The SUVmax was positively correlated with lesion diameter (r = 0.497, P < 0.001), while negatively correlated with the blood potassium level (r = -0.450, P < 0.001) and plasma renin activity (r = -0.297, P = 0.004). 63 cases of 73 PA patients with unilateral adrenal lesion were identified positive by 68Ga-pentixafor PET/CT, and 95.2 % of the 63 positive cases benefited from surgical resection of the identified positive lesions. Among 18 PA patients with bilateral lesions, 68Ga-pentixafor PET/CT identified positive lesions in 15 cases, and 86.7 % (13/15) of the positive cases benefited from total or partial adrenalectomy guided by 68Ga-pentixafor PET/CT. There was no significant difference in postoperative outcomes between patients undergoing partial adrenalectomy with those subjected to total adrenalectomy. The accuracy rate of 68Ga-pentixafor PET/CT in determining the dominant side of aldosterone secretion for PA was 85.7 %, which was comparable to the 71.4 % of adrenal vein sampling (AVS).
Conclusions: 68Ga-pentixafor PET/CT could effectively guide the surgical management for PA patients, achieving favorable postoperative outcomes. The accuracy rate of 68Ga-pentixafor PET/CT in identifying the dominant side of aldosterone secretion was not inferior to that of AVS.
Keywords: 68Ga-pentixafor PET/CT; Adrenalectomy; CXCR4 receptor; Primary aldosteronism.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Total or partial adrenalectomy for aldosterone-producing adenoma: can 68Ga-Pentixafor PET/CT predict surgical outcomes?Eur J Nucl Med Mol Imaging. 2025 Aug;52(10):3632-3642. doi: 10.1007/s00259-025-07244-9. Epub 2025 Apr 4. Eur J Nucl Med Mol Imaging. 2025. PMID: 40183955 Clinical Trial.
-
68Ga-pentixafor PET/CT Is a Supplementary Method for Primary Aldosteronism Subtyping Compared with Adrenal Vein Sampling.Mol Imaging Biol. 2025 Feb;27(1):142-150. doi: 10.1007/s11307-024-01976-0. Epub 2024 Dec 23. Mol Imaging Biol. 2025. PMID: 39715984 Free PMC article.
-
Typing diagnostic value of 68Ga-pentixafor PET/CT for patients with primary aldosteronism and unilateral nodules.Endocrine. 2025 Jan;87(1):314-324. doi: 10.1007/s12020-024-04024-7. Epub 2024 Sep 9. Endocrine. 2025. PMID: 39251468
-
Normotensive primary aldosteronism in a patient with myasthenia gravis: a localization diagnostic conundrum unraveled by 68Ga-pentixafor PET/CT - a case report with review of literature.Endocrine. 2025 Sep;89(3):704-709. doi: 10.1007/s12020-025-04311-x. Epub 2025 Jun 10. Endocrine. 2025. PMID: 40495043 Review.
-
Head-to-Head Comparison of 68Ga-PentixaFor PET/CT and FDG PET/CT for Detecting Hematologic and Solid Cancers: A Systematic Review and Meta-Analysis.AJR Am J Roentgenol. 2025 May 14. doi: 10.2214/AJR.25.32708. Online ahead of print. AJR Am J Roentgenol. 2025. PMID: 40366789 Review.
Cited by
-
Advances in Endocrine Tumor PET Imaging Targeting CXCR4 and GLP-1.Semin Nucl Med. 2025 Sep;55(5):766-775. doi: 10.1053/j.semnuclmed.2025.05.001. Epub 2025 May 29. Semin Nucl Med. 2025. PMID: 40447542 Review.
-
Editorial: Adrenal related hypertension: from bench to bedside, volume II.Front Endocrinol (Lausanne). 2025 Jul 3;16:1647120. doi: 10.3389/fendo.2025.1647120. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40678320 Free PMC article. No abstract available.
References
-
- Zennaro M.C., Boulkroun S., Fernandes-Rosa F.L. Pathogenesis and treatment of primary aldosteronism. Nat Rev Endocrinol. 2020;16(10):578–589. - PubMed
-
- Funder JW, Carey R.M., Mantero F., et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889–1916. - PubMed
-
- Williams T.A., Burrello J., Sechi L.A., et al. Computed tomography and adrenal venous sampling in the diagnosis of unilateral primary aldosteronism. Hypertension. 2018;72(3):641–669. - PubMed
-
- Lim V., Guo Q., Grant C.S., et al. Accuracy of adrenal imaging and adrenal venous sampling in predicting surgical cure of primary aldosteronism. J Clin Endocrinol Metab. 2014;99(8):2712–2719. - PubMed
LinkOut - more resources
Full Text Sources
