

Treatment-resistant Cushing disease and acromegaly in a young woman: A case of functional pituitary macroadenoma
- PMID: 39926265
- PMCID: PMC11802362
- DOI: 10.1016/j.radcr.2025.01.010
Treatment-resistant Cushing disease and acromegaly in a young woman: A case of functional pituitary macroadenoma
Abstract
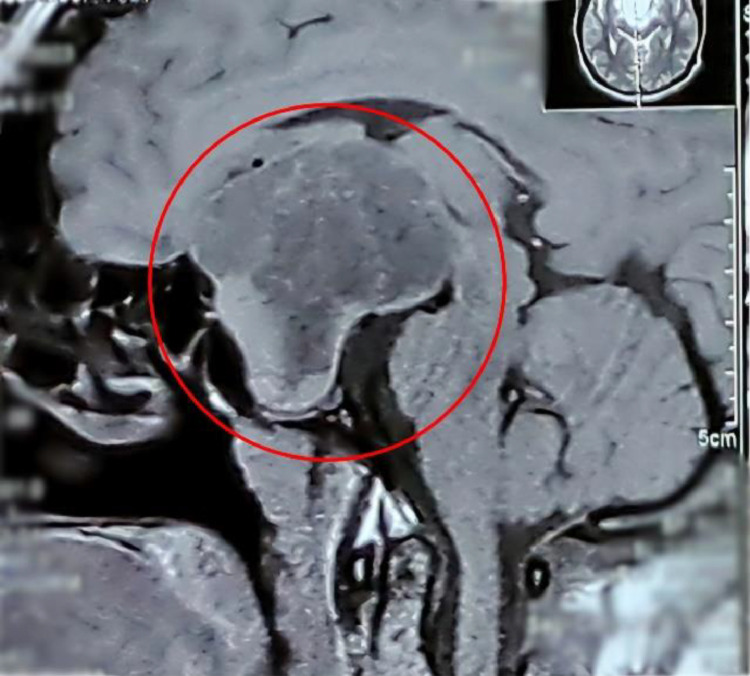
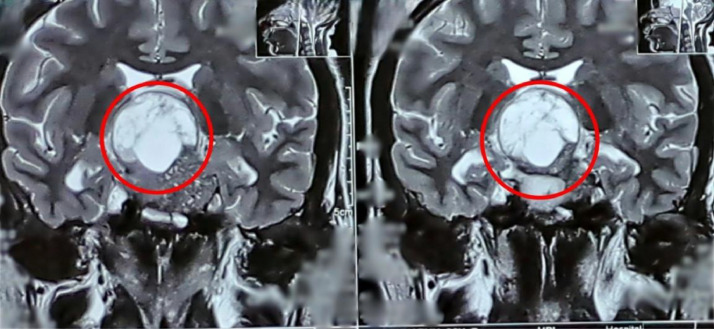
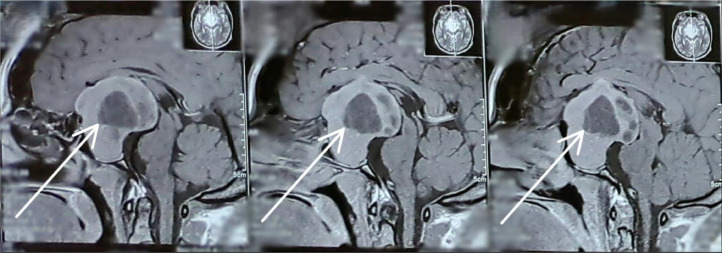
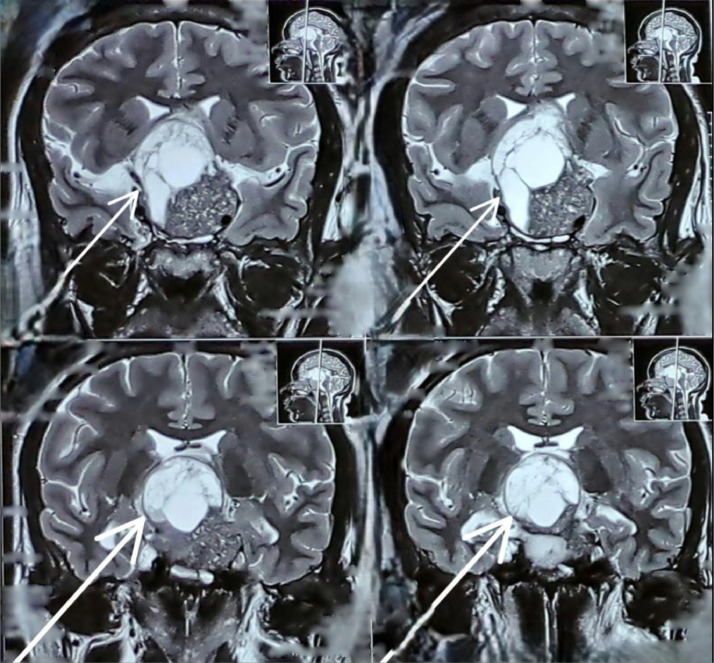
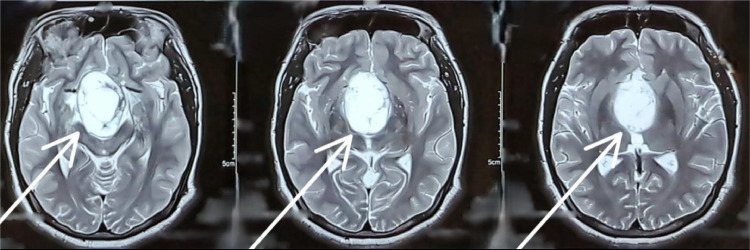
Cushing disease and acromegaly are common endocrine disorders caused by excessive cortisol and growth hormone production, respectively. Both conditions can co-occur due to functioning pituitary adenomas, which are typically benign pituitary gland tumors. This report discusses a 30-year-old woman with hyperpituitarism leading to treatment-resistant Cushing disease and acromegaly caused by a functional pituitary macroadenoma. A 30-year-old woman presented with a history of excessive weight gain, facial puffiness, fatigue, persistent headaches, and visual disturbances. Clinical examination revealed features consistent with Cushing disease and acromegaly, including a moon face, central obesity, and large hands and feet-the ophthalmologic evaluation identified bitemporal hemianopia, suggesting optic chiasm compression. Laboratory results showed elevated ACTH, IGF-1, and prolactin levels, alongside confirmed hypercortisolism. The patient also had secondary diabetes mellitus and galactorrhea-initial treatment with octreotide provided limited benefit, with persistent hormone elevations and insufficient symptom control. The patient underwent endonasal endoscopic transsphenoidal resection of the pituitary macroadenoma, leading to marked symptomatic and hormonal improvements. This underscores the diagnostic challenge and treatment complexity of such cases. Early diagnosis is critical for optimizing outcomes in patients with hyperpituitarism and mitigating complications. This case highlights the importance of multidisciplinary management and the necessity of long-term follow-up to monitor for recurrence and ensure sustained remission.
Keywords: Acromegaly; Cushing; Hormone; Macroadenoma; Microadenoma; Pituitary.
© 2025 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
Similar articles
-
Endoscopic Endonasal Surgery for Remission of Cushing Disease Caused by Ectopic Intracavernous Macroadenoma: Case Report and Literature Review.World Neurosurg. 2017 Feb;98:870.e5-870.e10. doi: 10.1016/j.wneu.2016.12.021. Epub 2016 Dec 18. World Neurosurg. 2017. PMID: 28003168 Review.
-
Digital analysis of hormonal immunostaining in pituitary adenomas classified according to WHO 2017 criteria and correlation with preoperative laboratory findings.Neurosurg Focus. 2020 Jun;48(6):E12. doi: 10.3171/2020.3.FOCUS2039. Neurosurg Focus. 2020. PMID: 32480373
-
A Rare Case When Acromegaly Meets Cushing Syndrome.JCEM Case Rep. 2023 Dec 19;2(1):luad145. doi: 10.1210/jcemcr/luad145. eCollection 2024 Jan. JCEM Case Rep. 2023. PMID: 38192880 Free PMC article.
-
Consecutive resections of double pituitary adenoma for resolution of Cushing disease: illustrative case.J Neurosurg Case Lessons. 2023 Nov 27;6(22):CASE23485. doi: 10.3171/CASE23485. Print 2023 Nov 27. J Neurosurg Case Lessons. 2023. PMID: 38011690 Free PMC article.
-
Outcomes of endoscopic transsphenoidal pituitary surgery.Endocrinol Metab Clin North Am. 2015 Mar;44(1):105-15. doi: 10.1016/j.ecl.2014.10.010. Epub 2014 Nov 4. Endocrinol Metab Clin North Am. 2015. PMID: 25732647 Review.
References
-
- Chanson P., Raverot G., Castinetti F., Cortet-Rudelli C., Galland F., Salenave S., French Endocrinology Society non-functioning pituitary adenoma work-group Management of clinically non-functioning pituitary adenoma. Ann Endocrinol (Paris) 2015;76(3):239–247. doi: 10.1016/j.ando.2015.04.002. Epub 2015 Jun 10. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
